16. October 2017
11 - 17. September 2017
Lille - Davis Cup Semifinals - Serbia vs. France
Official Dinner






12. September 2017
Lille - Davis Cup Semifinals - Serbia vs. France
Can't wait to absorb some incredible positive energy the upcoming week!
Looking forward to join the serbian Davis Cup by BNP Paribas team in a few hours!
On my way to Lille/France to support my friends at the semifinals tie Serbia vs. France.
Proud to be a member of one of the best national tennis teams of the world!

28. August - 10. September 2017
New York - US Open - Grand Slam
US Open with Doubles No. 1 Team in the world Melo/Kubot and Yen-Hsun Lu.

10 years - one team!
In New York at US Open Tennis Championships.
One of the tennis players I am working with this time is Yen-Hsun Rendy Lu and exactly this month we are celebrating 10 years of working together.
It has been an incredible journey so far, thank you Rendy for your trust in my work. Hopefully many more years to go!
I am happy that we could manage together every single injury situation in the quickest possible way over the past decade!
Special thanks to my mentor Klaus Eder and the whole team of EDEN REHA who also helped a lot over the years!
#TeamWork is the key


20. August 2017
New York - US Open - Grand Slam
Not a perfect but good week with the World No. 1 Doubles Team #MeloKubot in Cincinnati at Western & Southern Open.
Congrats to Lukasz on a new career high of No. 3 of the Emirates ATP World Tour Rankings!
Next stop New York City for US Open Tennis Championships!
Let's do this!

Just arrived to an amazing city!



18. August 2017
Cincinnati - Western & Southern Open - ATP 1000



11. August 2017
Montreal - Coupe Rogers - ATP 1000

08. August 2017
Montreal - Coupe Rogers - ATP 1000
Marriott Hotel Chateau Champlain

06. August 2017
Washington - Citi Open - ATP 500
Another good week with these guys in Washington.
Not the tournament win but runner-up at Citi Open!
An incredible 17-match winning streak ends today for team #MeloKubot, congrats on that!
Happy to be part of this amazing 2017 journey so far:
BNP Paribas Open Runner-up
Miami Open Win
Mutua Madrid Open Win
Ricoh Open Win
GERRY WEBER OPEN Win
Wimbledon Win
Citi Open Runner-up
World No. 1 and first team to qualify for Nitto ATP World Tour Masters (Tennis World Championships)
Off to Montreal for Coupe Rogers présentée par Banque Nationale! Let's do this!
Partner:
Blackroll® | Sportsline 運動前線 | Dynamic Tape | Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK | adidas
#Washington #WashingtonDC #CitiOpen #Physiotherapy #Osteopathy


05. August 2017
Washington - Citi Open - ATP 500
.


29. July 2017
Washington - Citi Open - ATP 500
Back in business at Citi Open with the Wimbledon champions!
Looking forward to the next weeks of hard work and lot's of fun at US OPEN series with the World No. 1 Doubles Team #MeloKubot! Let's do it!
Partner:
Blackroll® | Sportsline 運動前線 | Dynamic Tape | Premax | Voss Water | SEIRIN Corporation | Bounce Canada | adidas

23. July 2017
Taipei - Workshop
Thank you Sportsline 台灣 for your invitation and trust to talk in front of an amazing class for 2 days!
Enjoyed every minute!
Thank you to all my partners:
Sportsline 運動前線 | Blackroll® | Dynamic Tape | Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK
Man of the camera: Hsiao Photography
#Taipei #Taiwan #Sportsline #Blackroll #DynamicTape #Premax#VossWater #SportsPhysiotherapy #Tennis #Workshop #Lecture#Education #Physiotherapy #Osteopathy







21. July 2017
Taipei - Workshop
Final preparations for tomorrow's workshop with my translator, thank you Sportsline 台灣!
Only a few seats available!
You can register here:
職業網球 - 運動物理治療師研討會
Conference of Professional Sports Physiotherapist - Perspective in professional tennis
主辦單位:#sportslinetaiwan @sportslineasia
協辦單位:壢新醫院 - 聯新運動醫學中心
講者: @stefanduell
翻譯: 陳祐榕老師
日期:22-23, July 2017
報名辦法:
https://www.eventbrite.com/e/35134671749
22 July - 職業網球 - 運動物理治療師研討會 - Conference of Professional Sports-Physiotherapist for Tennis
23 July - 職業網球 - 運動物理治療師治療手法工作坊 - Workshop of Professional Sports Physiotherapist for Tennis
研討會簡介:
來自德國的運動物理治療師 Stefan Düll 擁有豐富的國家隊與運動賽事防護經驗,包含德國奧運代表隊、塞爾維亞國家隊甚至是中華台北代表隊都是他曾經服務的單位;而Stefan也是眾多網球職業選手的指定防護師例如職業網球球王祖高域,世界青少年網球第一的,世界職業網球排名第9位的,還有我們台灣最熟悉的盧彥勳(世界排名56)以及謝淑薇選手(最佳排名16)。 http://www.stefanduell.com/
Partner:
Blackroll® | Sportsline 運動前線 | Dynamic Tape | @Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK | adidas

20. July 2017
Taipei - Workshop
Just arrived at Taipei!
Happy to be back to this amazing city and am looking forward to my workshop this weekend!
You can join me for a 2-day education session for health professionals and fitness trainers, in which I will share a lot of practice-oriented insights into my work with professional tennis players, such as: how to prepare an athlete for a competition, how to provide acute treatment on court, how to support recovery, how to keep an athlete injury-free and a lot of further treatment tips and tricks out of my daily work to solve any kind of injury issues!
Additionally, I will introduce some very helpful tools which I use myself for my daily work with professional athletes: Blackroll® products, Dynamic Tape, Premax, SEIRIN Corporation or @PulsYoga.
Thank you @SportslineHK for the invitation. Looking forwards to it!
The course will be held in English and supported by a simultaneous translation into Chinese!
#Repost Sportsline 台灣
職業網球 - 運動物理治療師研討會
Conference of Professional Sports Physiotherapist - Perspective in professional tennis
主辦單位:#sportslinetaiwan @sportslineasia
協辦單位:壢新醫院 - 聯新運動醫學中心
講者: @stefanduell
翻譯: 陳祐榕老師
日期:22-23, July 2017
報名辦法:
https://www.eventbrite.com/e/35134671749
22 July - 職業網球 - 運動物理治療師研討會 - Conference of Professional Sports-Physiotherapist for Tennis
23 July - 職業網球 - 運動物理治療師治療手法工作坊 - Workshop of Professional Sports Physiotherapist for Tennis
研討會簡介:
來自德國的運動物理治療師 Stefan Düll 擁有豐富的國家隊與運動賽事防護經驗,包含德國奧運代表隊、塞爾維亞國家隊甚至是中華台北代表隊都是他曾經服務的單位;而Stefan也是眾多網球職業選手的指定防護師例如職業網球球王祖高域,世界青少年網球第一的,世界職業網球排名第9位的,還有我們台灣最熟悉的盧彥勳(世界排名56)以及謝淑薇選手(最佳排名16)。 http://www.stefanduell.com/
Partner:
BLACKROLL 台灣® | Sportsline 運動前線 | Dynamic Tape | Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK | Adidas Originals東區旗艦店
#Physiotherapy #Osteopathy

19. July 2017
Würzburg
#1
Happy to be part of this incredible 2017 journey so far:
BNPParibasOpen runner-up
Miami Open champion
Mutua Madrid Open champion
Ricoh Open champion
GERRY WEBER OPEN champion
Wimbledon champion
World No. 1
First team to qualify for Nitto ATP World Tour Masters (Tennis World Championships)
Big congrats Marcelo Melo and Łukasz Kubot!
Partner:
Blackroll® | Sportsline 台灣 | Dynamic Tape | Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK | adidas


17. July 2017
Würzburg
Just got back home from an very exciting Wimbledon working with Marcelo Melo and Łukasz Kubot who won the tournament!
Now preparing already for my workshop in Taipei/Taiwan which will be held on 22-23 of July 2017!
This time I am invited to hold a 2-day education session for health professionals and fitness trainers to provide them with the praxis-oriented insights into my work with professional tennis players, such as: how to prepare an athlete for a competition, how to provide acute treatment on court, how to support recovery, how to keep an athlete injury-free and a lot of further treatment tips and tricks out of my daily work to solve any kind of injury issues!
Additionally, I will introduce some very helpful tools which I use myself for my daily work with professional athletes: Blackroll® products, Dynamic Tape, Premax, SEIRIN Corporation or PulsYoga.
Thank you Sportsline 運動前線 for the invitation. Looking forward to it!
The course will be held in English and supported by a simultaneous translation into Chinese!
職業網球 - 運動物理治療師研討會
Conference of Professional Sports Physiotherapist - Perspective in professional tennis
主辦單位:#sportslinetaiwan Sportsline 台灣
協辦單位:壢新醫院 - 聯新運動醫學中心
講者: @stefanduell
翻譯: 陳祐榕老師
日期:22-23, July 2017
報名辦法:
https://www.eventbrite.com/e/35134671749
22 July - 職業網球 - 運動物理治療師研討會 - Conference of Professional Sports-Physiotherapist for Tennis
23 July - 職業網球 - 運動物理治療師治療手法工作坊 - Workshop of Professional Sports Physiotherapist for Tennis
研討會簡介:
來自德國的運動物理治療師 Stefan Düll 擁有豐富的國家隊與運動賽事防護經驗,包含德國奧運代表隊、塞爾維亞國家隊甚至是中華台北代表隊都是他曾經服務的單位;而Stefan也是眾多網球職業選手的指定防護師例如職業網球球王祖高域,世界青少年網球第一的,世界職業網球排名第9位的,還有我們台灣最熟悉的盧彥勳(世界排名56)以及謝淑薇選手(最佳排名16)。 http://www.stefanduell.com/
Partner:
BLACKROLL® | Sportsline 運動前線 | Dynamic Tape | Premax | SEIRIN Corporation | Voss Water | Bounce Canada | Bounce Balls UK
15. July 2017
London - Wimbledon - Grand Slam
Still under impression of being part of an incredible grass court season run with team #MeloKubot:
3 grass court tournaments, 3 grass court titles plus on top Wimbledon champions! Can't get better!
Congrats to Marcelo Melo and Łukasz Kubot on their 5th ATP World Tour title this year!
Also congrats to Lukasz on a new career high of No. 4 and Marcelo on breaking back to No. 1 of the Emirates ATP Rankings!

28. June 2017
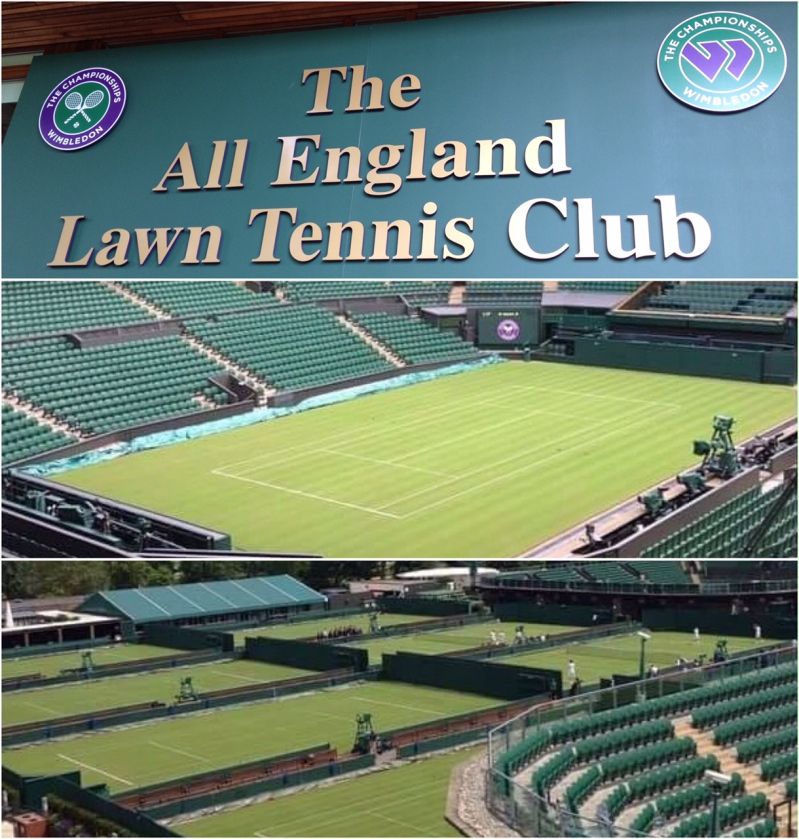
London - Wimbledon - Grand Slam
Just checked in at Wimbledon - it's always special to come back to 'The All England Lawn Tennis Club' to work with some of the world's best tennis players at the most important tennis tournament of the year!
Which tennis fan isn't dreaming about stepping at least once in a lifetime on one of this holy courts!?
Partner:
Blackroll® | Sportsline 運動前線 | Dynamic Tape | Premax | SEIRIN Corporationl | Bounce Canada | Bounce Balls UK
25. June 2017
Halle - Gerry Weber Open - ATP 500
2nd grass court tennis tournament, 2nd grass court tennis title!
Mission GERRY WEBER OPEN accomplished, another great week with this crew!
Congrats to Marcelo Melo and Łukasz Kubot on their 4th ATP World Tour crown this year!
Thank you to the whole team of Gerry Weber Open for a great tournament organization!
Off to London for the next and most important tennis tournament of the year - Wimbledon!

18. June 2017
Halle - Gerry Weber Open - ATP 500
Just arrived in Halle/Germany at GERRY WEBER OPEN.
Congrats on 25 years of ATP World Tour action!
Definitely one of the best #ATP500Series events!
17. June 2017
s`Hertogenbosch - RICOH Open - ATP 250
Mission Ricoh Open accomplished - another great week with this crew!
Congrats to Marcelo Melo and Łukasz Kubot on their 3rd ATP World Tour title this year - great job!
Thank you to the whole team of Ricoh Open for a great tournament organization!
Off to Halle/Germany for the next tournament GERRY WEBER OPEN!

15. June 2017
s`Hertogenbosch - RICOH Open - ATP 250
LOWER CROSSED SYNDROME (LCS) SERIES 18/19 - ACTIVATION OF THE GLUTEUS MUSCLES - COOK BRIDGE
Your glutes are an incredibly important muscle group for many reasons, including preventing injury and improving performance!
This is why it is essential to do exercises with which you can get your glutes properly fired up and working for you. These will help you move better, feel better, and kick your training up to another level!
We started with the 'Glute Bridge', which is an excellent starting point, but most of you will quickly need to move on to more challenging variations to really get your glutes fired up. The next step would be the 'Cook Bridge/Cook Hip Lift' - Developed by physical therapist Gray Cook, this exercise eliminates lumbar spine movement, forcing the work to happen at the glutes.
How to do this movement:
1-Get into the bridge position.
2-Place a tennis ball below your bottom rib on one side, and hug the same knee to your chest, pinning the ball down with your thigh.
3-Holding onto this position, lift your hips in the air, and repeat.
4-Repeat this about 15-20 times, ensuring your hips remain stable throughout the entire exercise. Then change the side.
This exercise is essential and should be included in a good warmup routine before any workout!
Additionally this exercise can help if you suffer from lower back pain!
LOWER CROSSED SYNDROME (LCS) SERIES 19/19 - ACTIVATION OF THE GLUTEUS MUSCLES - GLUTE BRIDGE WITH MARCH
Your glutes are an incredibly important muscle group for many reasons, including preventing injury and improving performance!
This is why it is essential to do exercises with which you can get your glutes properly fired up and working for you. These will help you move better, feel better, and kick your training up to another level!
We started with the 'Glute Bridge' followed by the 'Cook Bridge/Cook Hip Lift'. The next step would be 'Glute Bridge With March' - This one forces you to engage all of your stabilizer muscles.
How to do the glute bridge with march:
1-Get in to the bridge position and lift your hips in the air.
2-At this top position, and without allowing any movement at your hips, slowly lift one leg off the ground and hold for two seconds.
3-Put it down and lift the opposite leg.
4-Repeat this about 15-20 times, ensuring your hips remain stable throughout the entire exercise.
This exercise is essential and should be included in a good warmup routine before any workout!
Additionally this exercise can help if you suffer from lower back pain!
11. June 2017
s`Hertogenbosch - RICOH Open - ATP 250
LOWER CROSSED SYNDROME (LCS) SERIES 14/19 - MYOFASCIAL RELEASE OF THE GLUTEUS MUSCLES
From my previous post you know the result of lower crossed patterns is an inhibition of the glute muscles.
These muscles (gluteus maximus, medius and minimus) are main stabilizer of the pelvis and also help level the pelvis therefore they control every joint below them, including the ankle/foot.
They are essential for hip, pelvis and low back stability and balance each time our foot hits the ground, thats why it is very important to work on a proper activation of these important structures!
Before working on activation of the glute muscles I try to release them with several myofascial treatment techniques.
Glute muscle trigger points can lead to referred pain in the gluteal region and leg similar like sciatica.
On the picture you can see how I approach the glute muscles to perform a myofascial treatment as:
1 - a trigger point technique: make sure you hold the pressure as long the patient tells you the pain or the radiation goes down or the pain is not radiating anymore but at least for 1 minute and finish the technique then with a Ponçage. I usually hold the pressure until i feel a myofascial release under my fingers!
2 - a fascial release technique for the complete glute muscles: make sure you perform the technique from proximal to distal or distal to proximal along each muscle stomach.
3 - a release technique between the glute max muscle and the posterior hip muscles: use the elbow from one arm and the hand from your other arm is moving the hip in internal and external rotation, stay with your elbow on the spot until you feel a fascial release!
How to activate the glute muscles I will discuss in my following post!
LOWER CROSSED SYNDROME (LCS) SERIES 15/19 - GLUTEUS MAXIMUS MUSCLE SELF-RELEASE EXERCISE
Why are the glutes so inactive?
- The first and most common reason people suffer from underactive glutes is due to lifestyle. Even when people train hard every day, if they spend the majority of the remainder of the day sitting down, then they are simply not using their glutes!
- Another common reason for glutes not working properly is due to injury. Often an injury happens that changes the mechanics and motor programming of a person’s body. This can lead to some muscle groups becoming overactive, while others become underactive.
- A 3rd common reason I see glutes that aren’t working properly is due to trigger points or fascial tightness which disturbs the intramuscular coordination (quality of muscle contraction) and therefore the ability to contract the full muscle properly.
That's why you should always make sure: Before you start activating your gluteus maximus, free it of trigger points and fascial tightness with the exercises you can see in the video.
You take a Blackroll® BALL, Lacrosse ball, Base- or Tennisball. Place it below your gluteus maximus and try the release exercise which you can see in the upper video.
Or you take a @BLACKROLL® and roll slowly among the muscle (lower video), trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease.
These exercises are essential and should be included in a good warmup routine before any workout!
Additionally these exercises can also help if you suffer from lower back pain!
How to activate these important structures I will discuss in my following posts!
LOWER CROSSED SYNDROME (LCS) SERIES 16/19 - GLUTEUS MEDIUS MUSCLE SELF-RELEASE EXERCISE
The glute med stabilizes the pelvis when you walk or run and abducts the leg away from the body.
A common reason I see glutes that aren’t working properly is due to trigger points or fascial tightness which disturbs the intramuscular coordination (quality of muscle contraction) and therefore the ability to contract the full muscle properly.
That's why you should always make sure: Before you start activating your gluteus medius muscle free it of trigger points and fascial tightness with the exercises you can see in the video.
You take a Blackroll® BALL, Lacrosse ball, Base- or Tenniaball. Place it lateral, below the iliac crest and try the release exercise which you can see in the upper video (Adduction/Abduction of the hip).
Or you take a @BLACKROLL® and roll slowly among the muscle (lower video), trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Ensuring you roll from the origin to the insertion is a good way to target the entire length of the muscle.
These exercises are essential and should be included in a good warmup routine before any workout!
Additionally these exercises can also help if you suffer from lower back pain!
How to activate these important structures I will discuss in my following posts!
LOWER CROSSED SYNDROME (LCS) SERIES 17/19 - ACTIVATION OF THE GLUTEUS MUSCLES - GLUTE BRIDGE
From my previous posts you know the result of lower crossed patterns is an inhibition of the glute muscles.
These muscles (gluteus maximus, medius and minimus) are main stabilizer of the pelvis and also help level the pelvis therefore they control every joint below them, including the ankle/foot.
They are essential for hip, pelvis and low back stability and balance each time our foot hits the ground, thats why it is very important to work on a proper activation of these important structures!
We start with the 'Glute Bridge':
This is a great, functional exercise! The basic glute bridge is simple, just lay on your back with your knees bent, lifting your hips in the air. Repeat this about twenty times, ensuring your hips remain stable throughout the entire exercise.
This is an excellent starting point, but most of you will quickly need to move on to more challenging variations to really get your glutes fired up which I will show in the following posts.
1 - Glute Bridge
2 - Glute Bridge with Mini-Band - More activation for gluteus medius and minimus muscle
This exercise is essential and should be included in a good warmup routine before any workout!
Additionally this exercise can help if you suffer from lower back pain!
29. May 2017
Paris/Roland Garros - French Open - Grand Slam
LOWER CROSSED SYNDROME (LCS) SERIES 11/19 - LOW BACK ERECTOR MUSCLES
The erector spinae muscle group runs along the spine from the iliac crest of the pelvis all the way to the neck. The region we are talking about regarding the LCS is the low back portion of the erector spine muscle group.
The low back erectors tend to get facilitated and overused. They tend to dominate and do too much in any given movement pattern (just like the hip flexor group). They often do this at the expense of the glutes, which is a big problem. Like in my first posts mentioned, when your low back erectors think they're your glutes...we have dysfunction and a big problem!
The glutes, which will be discussed in the next posts, act to stabilize and level the pelvis to prevent it from being pulled into too much anterior pelvic tilt (and low back hyperextension). When the low back extensors are doing too much, they take over for the glutes and this puts us into too much extension over time which leads to lower back problems.
Again, sitting is a big contributor:
It places our pelvis in a bad position, and fires on the extensors to work when the glutes are sleeping and weakened.
This extensor dominant pattern shows up elsewhere and affects athletic performance, sports etc.
Even high level athletes can be victims of this!
LOWER CROSSED SYNDROME (LCS) SERIES 12/19 - MYOFASCIAL TREATMENT OF THE LOW BACK ERECTOR MUSCLES
The muscles of the back can be divided into three groups – superficial, intermediate and intrinsic:
- Superficial – associated with movements of the shoulder.
- Intermediate – associated with movements of the thoracic cage.
- Deep – associated with movements of the vertebral column. The deep muscles develop embryologically in the back, and are thus described as INTRINSIC muscles. The deep muscles of the back are well-developed, and collectively extend from the sacrum to the base of the skull. They are associated with the movements of the vertebral column, and the control of posture. Anatomically, the deep back muscles can be divided into three layers: superficial, intermediate and deep.
The superficial muscles are also known as the spinotransversales. There are two muscles in this group: splenius capitis and splenius cervicis.
There are three intermediate intrinsic back muscles – the iliocostalis, longissimus and spinalis. Together these muscles form a column, known as the erector spinae. The erector spinae is situated posterolaterally to spinal column, between the vertebral spinous processes and the costal angle of the ribs.
All three muscles can be subdivided by their superior attachments, into: lumborum, thoracic, cervicis and capitis.
The deep intrinsic muscles are located underneath the erector spinae. They are a group of short muscles, associated with the transverse and spinous processes of the vertebral column. There are three major muscles in this group: the semispinalis, multifidus and rotatores.
The low back erectors tend to do too much in LCS which leads to stiffness and trigger points. That's why it is very important to apply a proper myofascial release treatment on these structures. Usually I do not use a lot of treatment devices, but in this case the 'Small Bevelled-Tip T-BAR' is very useful!
On the picture you can see several myofascial release techniques for the low back erector muscles!
LOWER CROSSED SYNDROME (LCS) SERIES 13/19 - GLUTEUS MAXIMUS
The gluteal muscles all have important functions but these muscles are often inhibited in people and even athletes we see in our daily treatment sessions. The glute max extends and externally rotates the hip. It also helps level the pelvis and control every joint below them, including the ankle/foot.
They are essential for hip, pelvis and low back stability and balance each time our foot hits the ground.
As you can see in the picture, the glutes act to counteract anterior pelvic tilt (and the associated low back hyperextensjon). They work along with the core to create a neutral spine. The glutes and core work together so we can brace efficiently when we need to, in order to create a neutral stable spine and torso.
The problem is the glutes often are off, they stop working along with the core and we begin to lose our ability to stable efficiently. This happens both statically and dynamically. A neutral braced spine means efficient power output, efficient movement, more mobility, better posture, less prone to pain/injury.
And again, sitting is a big contributor why our glutes are inhibited. They are meant to be on fire a lot, working when we are on our feet. They are completely turned off when we sit, sitting basically squishes the glute tissues. The result is tight and restricted hips, excessive tone in the muscles around the hips, and poor overall tissue quality!
That is a very big problem in our today's society! If I find this problem I usually free the glutes from trigger points and fascial tightness and then I try to wake them up which I will show in my following posts!
The gluteal muscles all have important functions but these muscles are often inhibited in people and even athletes we see in our daily treatment sessions. The glute max extends and externally rotates the hip. It also helps level the pelvis and control every joint below them, including the ankle/foot.
They are essential for hip, pelvis and low back stability and balance each time our foot hits the ground.
As you can see in the picture, the glutes act to counteract anterior pelvic tilt (and the associated low back hyperextensjon). They work along with the core to create a neutral spine. The glutes and core work together so we can brace efficiently when we need to, in order to create a neutral stable spine and torso.
The problem is the glutes often are off, they stop working along with the core and we begin to lose our ability to stable efficiently. This happens both statically and dynamically. A neutral braced spine means efficient power output, efficient movement, more mobility, better posture, less prone to pain/injury.
And again, sitting is a big contributor why our glutes are inhibited. They are meant to be on fire a lot, working when we are on our feet. They are completely turned off when we sit, sitting basically squishes the glute tissues. The result is tight and restricted hips, excessive tone in the muscles around the hips, and poor overall tissue quality!
That is a very big problem in our today's society! If I find this problem I usually free the glutes from trigger points and fascial tightness and then I try to wake them up which I will show in my following posts!
28. May 2017
Paris/Roland Garros - French Open - Grand Slam
LOWER CROSSED SYNDROME (LCS) SERIES 1/19
Upper and Lower Crossed Syndromes are two of the most common aberrant postural patterns. Today's therapist benefit from working with Janda's upper and lower, or proximal-and-distal, crossed syndrome theory when dealing with clients who suffer from neck or back pain!
Lower Crossed Syndrome (LCS):
This 'swayback' posture typically develops from prolonged sitting and sleeping with knees and hips flexed. As lumbar and SI-Joints become fixated, protective spasm further compresses the spine causing low back, hip and leg pain. Therapists must restore balance and symmetry to all lower crossed muscles and re-check firing order patterns in hip extension, hip flexion and hip abduction!
The tight line (A = Tight Line) travels through the iliopsoas and lumbar erectors, which pull and hold this aberrant swayback posture. Reciprocal inhibition weakens the abdominals and gluteals (B = Weak Line) allowing this dysfunctional pattern to develop.
In this lower crossed pattern, the short iliopsoas muscles anteriorly tilt the pelvis, creating excessive lumbar lordosis while erector spinae myofascial contractures hold this "bowing" pattern. The weak abdominals and gluteals, unable to stabilize the pelvis, allow this aberrant swayback pattern to develop. Local and referred pain symptoms appear as compressive forces disrupt normal functioning of facet joints, discs and spinal ligaments.
Connecting the abdominals and gluteals, weak line B permits the lower crossed asymmetry. Core support is lost as the stretch-weakened rectus and transversus abdominal muscles are overpowered by the pull of the strong iliopsoas and erector spinae groups. Muscles listed below also contribute to distortion and compression of the body's bony framework leading to pain-spasm-pain cycles. Myoskeletal Techniques effectively restore balance and symmetry by manually lengthening muscles of the tight line and 'spindle-stimulating' neurologically inhibited muscles of the weak line. Credit goes to Vladimir Janda, MD for research and development of the Upper and Lower Crossed Syndromes.
Still, a frustrating question remains: Why do so many clients present with this lower crossed pattern?
The last century has witnessed a dramatic acceleration in our culture's flexion addiction. This pervasive and insidious condition is primarily due to the population's generational transition from an active group of movers to a sedentary bunch of sitters. Researchers estimate that up to 75 percent of chronic neck/back pain clients will present with one or both of these crossed patterns.
Typical muscle imbalances in the LCS:
Tight/Facilitaded:
Iliopsoas, Rectus femoris, Hamstrings, Erector spinae, Tensor fascia lata, Thigh adductors, Piriformis, Quadratus lumborum, Gastrocnemius/Soleus
Weak/Inhibited:
Rectus abdominis, Transversus abdominis, Obliques, Gluteus Maximus, Gluteus medius/minimus, Vastus lateralis/medialis, Tibialis anterior
https://www.instagram.com/p/BUovaBggSfV/?taken-by=stefanduell
LOWER CROSSED SYNDROME (LCS) Series 2/19 - TIGHT/FACILITATED HIP FLEXORS
The hip flexor muscle group gets a lot of attention because it is common to have dysfunction at the LCS. The iliopsoas is the main hip flexor muscle, however the TFL, Sartorius, and Rectus femoris (Quad) also act as hip flexors.
The iliopsoas has a vital role in everyday activities like walking and running. The psoas originates at the lumbar spine and connects with the iliacus to insert on the femur. Because of this, it is often a cause or contributor to low back pain, pelvic/hip instability, problems with maintaining a neutral spine etc. It functions as a powerful hip flexor and a stabiliser of the spine and trunk during other movements.
The Iliopsoas is generally tight on most people in our sitting society. When we sit, the hip flexors are stuck in a shortened position at around 90°, often for long periods of time. A lot of excess tone and tissue tension often results, and this can lead to dysfunctional movement and mobility issues.
All hip flexors tend to get brutally tight and facilitated. They develop a ton of muscle tension, and also are the first ones to jump in and dominate a movement.
The more dominant these muscles become, the more they influence our pelvis and therefore our posture and positioning. They tend to jump in and take over for the deeper stability muscles, especially when the body is searching for stability. This leads to further weakness and inhibition of the deep core and stability muscles that are very important for postural integrity.
Tight, restricted and overregulated hip flexors can lead to:
▪️inhibited glutes, since they do the exact opposite and are the primary hip extensors.
▪️taking over and act like the core, which is supposed to be stabilizing the lumbo-pelvic region.
▪️weakness, especially in ranges above chair level…this means they don't know what to do in deep hip flexion movements such as the squat.
▪️big problems in athletics as they play an important role in movement.
https://www.instagram.com/p/BUqhJKzA8RO/?taken-by=stefanduell
LOWER CROSSED SYNDROME (LCS) SERIES 3/19 - MYOFASCIAL TREATMENT OF THE ILIOPSOAS MUSCLE
The iliopsoas muscle belongs to the inner hip muscles and is innervated by the femoral nerve + lumbar plexus. It consists of:
▪️Psoas major: origin. from 1st-4th lumbar vertebrae, costal processes of all lumbar vertebrae and 12th thoracic vertebrae + ins. at the lesser trochanter of the femur.
▪️Iliacus: runs from the iliac fossa to the lesser trochanter.
The psoas major and iliacus unify in the lateral pelvis shortly before the inguinal ligament becoming the iliopsoas. There they pass below the inguinal ligament through the muscular lacuna together with the femoral nerve. Both muscles are completely surrounded by the iliac fascia. The lumbar plexus lies dorsally from the psoas major which is penetrated by the genitofemoral nerve.
The iliopsoas is the strongest flexor of the hip joint (important walking muscle). In the supine position it decisively supports the straightening of the upper body (e.g. during sit-ups). Furthermore it rotates the thigh laterally. A unilateral contraction leads to a lateral flexion of the lumbar vertebrae column. It plays a significant role in the movement and stabilization of the pelvis.
On the picture you can see how I approach the iliopsoas to perform a myofascial treatment as:
1-a trigger point technique: make sure you hold the pressure as long the patient tells you the pain or the radiation goes down or the pain is not radiating anymore but at least for 1 minute and finish the technique then with a Ponçage. I usually hold the pressure until i feel a myofascial release under my fingers!
2-a fascial release technique for the complete iliopsoas: make sure you perform the technique from proximal to distal or distal to proximal along the muscle stomach.
3-a release technique between the psoas and iliacus: use the thumb from one hand and your finger 2-5 from the other hand and stay between both muscles until you feel a fascial release!
https://www.instagram.com/p/BUrq5HYANNo/?taken-by=stefanduell
LOWER CROSSED SYNDROME (LCS) SERIES 4/19 - ILIOPSOAS MUSCLE SELF-RELEASE TECHNIQUE
The iliopsoas has a vital role in everyday activities like walking and running. The psoas originates at the lumbar spine and connects with the iliacus to insert on the femur. Because of this, it is often a cause or contributor to low back pain, pelvic/hip instability, problems with maintaining a neutral spine etc.
It functions as a powerful hip flexor and a stabiliser of the spine and trunk during other movements. It has an important role with breathing as it attaches to the diaphragm and therefore gets affected during emotional and physical stress. Psoas is also known as the muscle of fear… Prolonged stress means a contracted or tight posas muscle!
The Iliopsoas is generally tight on most people in our sitting society. When we sit, the hip flexors are stuck in a shortened position at around 90°, often for long periods of time. A lot of excess tone and tissue tension often results, and this can lead to dysfunctional movement and mobility issues.
A tight iliopsoas will compress the spine, if it is on one side tighter than on the other it will compress on the same side of the spine and damaging the joints on that side + squeezing the disc to the opposite direction.
In the video you can see how to perform a self-release technique for the iliopsoas muscle: you take a Blackroll® BALL, Lacrosse ball or Tennisball + a Kettlebell. Place it at the third of a distance between ASIS and umbilicus, then perform the exercise as shown in the video for 30 seconds to 2 minutes per side. Please be careful with this exercise, consult your physician before doing this.
If you have back, hip, or knee pain… releasing the psoas muscle is almost always beneficial and may result as immediate pain relief and levelling of the pelvis!
https://www.instagram.com/p/BUtFF-qARqB/?taken-by=stefanduell
LOWER CROSSED SYNDROME (LCS) SERIES 5/19 - ILIOPSOAS MUSCLE STRETCHING
The iliopsoas has a vital role in everyday activities like walking and running. It connects the spine to the lower extremity. It functions as a powerful hip flexor and a stabiliser of the spine and trunk during other movements. It has an important role with breathing as it attaches to the diaphragm and therefore gets affected during emotional and physical stress. Psoas is also known as the muscle of fear… Prolonged stress means a contracted or tight posas muscle!
The Iliopsoas and QL muscles are generally tight on most people in our sitting society. A tight iliopsoas and QL will compress the spine when they become tight! If both are on one side tighter than on the other it will compress on the same side of the spine and damaging the joints on that side + squeezing the disc to the opposite direction.
In the video you can see a simple and common exercise that, when combining with an active posterior pelvic tilt, will perfectly stretch the hip flexor in the front of the hip!
You can combine the stretch with a side bend to stretch some of the oblique and lower back (QL).
Hold each side for 1-2 minutes and don’t stop breathing! Breath deep into your stomach and therefore your thoracic diaphragm!
LOWER CROSSED SYNDROME (LCS) SERIES 6/19 - DEEP ABDOMINAL MUSCLES / CORE MUSCLES
A very obvious result of lower crossed patterns is an inhibition of the core or deep abdominal muscles.
The key muscles that make up the core are the deep abdominals (transverse abdominus and obliques), pelvic floor, and diaphragm. As you can see in the picture, these muscles enclose the midsection and help create a girdle of support to stabilize the torso.
The most important role of the core muscles is to provide stability to the body. Stability in stance, while moving, while running, while playing sports etc.!
But they can only provide stability if they are in a good position to work well and when they are not inhibited.
The problem is, they tend to get inhibited over time if we aren't used to using them for stability, and when we can't align ourselves properly in order to use them. The more we sit, the more they tend to get inhibited as the muscles I talked about in my previous posts get facilitated.
Another problem is that most of the people don’t know how to activate and work on this muscles, which I will show you in my next post!
When working, these muscles provide stability and keep the torso upright. They keep the ribcage stacked on top of the pelvis, and they help maintain a neutral spine. When the body is in neutral and upright, our prime stabilizers can work to do their job so that the prime movers can actually move us safely and efficiently!
LOWER CROSSED SYNDROME (LCS) SERIES 7/19 - MYOFASCIAL RELEASE OF THE RECTUS ABDOMINIS MUSCLE
From my previous post you know the result of lower crossed patterns is an inhibition of the core or deep abdominal muscles.
These muscles (transverse abdominis, obliques, pelvic floor, diaphragm) are main stabilizer of the body, thats why it is very important to work on a proper activation of these important structures!
Before working on activation of the core muscles I always release the rectus abdominis muscle with several myofascial treatment techniques as you can see in the picture.
A tight or shorten rectus abdominis can lead to muscle imbalances and therefore to lower back problems!
Rectus abdominis muscle trigger points can lead to referred pain in stomach, thigh and lower back!
How to activate the core muscles I will discuss in my following posts!
LOWER CROSSED SYNDROME (LCS) SERIES 8/19 - ACTIVATION OF THE CORE MUSCLES
Very important for every athlete to prevent injuries as well as for everyone who is suffering from lower back or lower extremity problems!
People with low back pain, past and present, have been shown to have poor motor control and activation of their transversus abdominis (TrA) and multifidus (MF) muscles.
First, what do these muscles do? They work with the diaphragm and pelvic floor to adjust the intraabdominal pressure - affecting the spine stability - and control intersegmental motion of the spine. Meaning they help keep your spine in the right place!
TrA and MF are active during all functional tasks. The central nervous system (CNS) sends messages to activate these muscles before predictable movements, and to react to unexpected movements. So the right timing in use of these muscles is important!
Working on your TrA and MF activation is an important step in improving and preventing that annoying recurring low back pain.
Good muscular control of the core and spine can help reduce instability and pain!
These exercises, which are best learned with a physical therapist, consist of the following:
1-Finding the position the spine is most comfortable in (neutral spine)
2-Educating the back muscles to keep the spine in the neutral position (MF muscles)
3-Educating how to contract the TrA muscle
4-Educating how to contract the pelvic floor
5-Educating how to contract the thoracic diaphragm
6-Maintaining the neutral position through a series of movements that apply more and more degrees of freedom of motion.
Dynamic lumbar stabilization exercises are commonly prescribed for any kind of lumbar problems and even for reducing sciatica-type pain from degenerative disc disease, or pain that radiates into the buttock and/or down the back of the leg.
LOWER CROSSED SYNDROME (LCS) SERIES 9/19 - STRENGTHENING OF THE CORE MUSCLES - EXERCISE VARIATION
Regarding my previous post about 'Activation of the Core Muscles' I wanted to show some more exercises which are very helpful if you suffer from inhibited core muscles because of 'Lower Crossed Syndrome' or even from back problems in general!
Mobility, Flexibility and Stability of the spinal system are very important aspects to watch at! The 'Lower Trunk Rotation' and 'Upper Trunk Rotation' exercises as shown on the picture can help to manage it!
Don't forget to activate your Core Muscles before you start doing this exercises but also in general before exercising like I explained in the previous post.
Good neuro-muscular control of the core and spine is the key!
My client Yen-Hsun Rendy Lu was able to stabilize a lumbar disc protrusion L3-L4 playing professional tennis and avoiding a lower back surgery by following this training strategy!
https://www.instagram.com/p/BU14m9YAw0s/?taken-by=stefanduell
LOWER CROSSED SYNDROME (LCS) SERIES 10/19 - STRENGTHENING THE CORE MUSCLES - NEXT LEVEL CORE TRAINING
Low back stability is a skill that must be trained. These drills by @vitasphysio show some great stability especially anti rotation.
TRAIN FOR STABILITY, NOT INSTABILITY!
Trade oblique crunches for these dynamic oblique holds to create a bombproof core. Rather than teaching the obliques to rotate the spine out of neutral, teach it to maintain neutral and resist the rotation.
A stable, neutral spine is less prone to disc herniations and quadratus lumborum muscle overuse injuries. It's all about good posture under load!
Remember to take your time and focus on form! Twisting during this exercise defeats the purpose!
SET UP PROPERLY!
To set up safely (without rotation), keep the shoulders retracted while shifting the hands to the side. The weight of the dumbbells will eventually surpass your center of gravity and tilt your entire body on its side. It's important to already have the core braced prior to starting as this will prevent overshooting the distance and completely tipping over.
23. May 2017
Paris/Roland Garros - French Open - Grand Slam
Back at work:
17. May 2017
THORACIC OUTLET SYNDROME SERIES 1/9: Thoracic Outlet Syndrome (TOS) and Self-Treatment
TOS are a group of syndromes involving pressure on the brachial plexus.
Each syndrome is named according the structure that is causing the compression.
1-SCALENE ANTERIOR SYNDROME:
The fibres of the brachial plexus must pass through a narrow aperture between scalenes anterior and medius. Any increased tone in one of these muscles (usually anterior), will provide enough compression to produce symptoms. Scarring and adhesions from injuries can be causes of compression, particularly if found at the attachments of the scalenes. Dysfunction or misalignent of the cervical spine may also be a contributing factor to this syndrome.
2-PECTORALIS MINOR SYNDROME (HYPERABDUCTION SYNDROME): In this case, the compression occurs where the neurovascular bundle passes between the tendon of pectoralis minor and the coracoid process of the scapula. Tractioning is greatest with the arm in abduction, but even with the arm dependent, enough pressure from postural problems or tight pectoralis muscles can cause symptoms.
3-COSTOCLAVICULAR SYNDROME:
Symptoms result in this case when the neurovascular bundle is tractioned between the clavicle and the first rib. This is often bilateral, indicating a symmetrical postural cause.
CAUSES:
Crutch use; Joint subluxation; Adhesions and scarring; Muscular hypertonicity from postural dysfunction such as hyperkyphosis; Trigger points; Occupational stresses; Emotion stresses; All of which lead to shallow breathing and poor sleeping posture.
SIGNS AND SYMPTOMS:
All thoracic outlet syndromes feature paraesthesia in the arm, forearm, hand, and fingers. Symptoms are usually unilateral, but can be bilateral, particularly if postural dysfunction is a main cause.
Anterior scalene syndrome is also noted for edema in the hands and fingers.
On the picture you can see several exercises which can help if you suffer from TOS!
https://www.instagram.com/p/BUMv0R7gl0R/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 2/9: SCALENE ANTERIOR SYNDROME
Regarding my yesterday's post about the Thoracic Outlet Syndrome (TOS) I wanted to show some treatment techniques on how to solve the SCALENE ANTERIOR SYNDROME -> MYOFASCIAL RELEASE OF THE SCALENE MUSCLES AND STERNOCLEIDOMASTOID MUSCLE
Anatomy:
The fibres of the brachial plexus and the subclavian artery must pass through a narrow aperture between anterior and middle scalene muscle. -> If this aperture makes a problem it can lead to paresthesia or weakness in the upper limb.
The fibres of the subclavian vein, the suprascapular vein, the transverse cervical vein and the phrenic nerve must pass through a narrow aperture between the anterior scalene muscle and the sternocleidomastoid muscle. -> If this aperture makes a problem it can lead to edema in the hands/fingers and also to problems with the thoracic diaphragm.
The fibres of the long thoracic nerve must pass through a narrow aperture between middle and posterior scalene muscle. -> If this aperture makes a problem it can lead to a problem with the serratus anterior muscle.
Any increased tone in one of these muscles (usually scalene anterior), will provide enough compression to produce symptoms. Scarring and adhesions from injuries can be causes of compression, particularly if found at the attachments of the scalenes. Dysfunction or misalignent of the cervical spine may also be a contributing factor to this syndrome.
Active trigger points in the scalene muscles can mimic a TOS and initiate similar symptoms, often characterized by numbness or tingling in the thumb or index finger.
On the picture you can see several myofascial release techniques for the scalene muscles as well as for the sternocleidomastoid muscle.
https://www.instagram.com/p/BUOK-4fA8Yc/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 3/9: SCALENE ANTERIOR SYNDROME SELF-TREATMENT
As a follow up to my previous post about the SCALENE ANTERIOR SYNDROME I wanted to show how you can perform a self-treatment to release tension in the scalene muscles and in the sternocleidomastoid muscle (SCM).
Relieving tension can be done using a Blackroll® TWISTER, Lacrosse ball, Tennisball or even your thumbs.
Especially the BLACKROLL® TWISTER is very useful as it does not only work with applying body weight to it but also allows the combination of pressure and twisting. The result: circulation rises, trigger bands and -points are stimulated and the fascial tissue becomes well hydrated:
Make sure to find the right tension areas of the scalene muscles and SCM and apply good pressure into the muscle. Then you can twist it and move your head while the TWISTER or ball is pressed in. For the right SCM you rotate/extend your cervical spine to the left side and for the right scalene muscles you side band your cervical spine to the left side. 1-2 minutes per side is good for the beginning. For the muscles on the left you just perform it to the opposite.
How to find the SCM and scalene muscles? The SCM attaches to the sternum + clavicel and travels up to your mastoid process (right behind the ear). To localize the right SCM you turn your head to the left, look down and you can palpate the prominent muscle stomach of the SCM perfectly. The scalene muscles are located right behind the SCM, they originate from the transverse processes from the cervical vertebrae of C2 to C7 and insert onto the first and second ribs.
In the left video you can see a myofascial self-treatment release techniques for the SCM and in the right video for the scalene muscles.
https://www.instagram.com/p/BUPMvpsgjK0/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 4/9: PECTORALIS MINOR SYNDROME
.
The pec minor originates on the coracoid process on the front of the scapula and splits into three sections that travel diagonally downward and medial to attach to the 3rd to 5th ribs.
.
Contraction of the pec muscle pulls the shoulder blade downward (depression) and forward (protraction) on the ribcage. Conversely, if the shoulder is held in place by the levator scapula and trapezius muscles, contraction of the pectoralis minor can elevate the upper ribcage and assist in inhalation.
.
Chronic tension in the pectoralis minor can produce “winging of the scapula” in which the vertebral edge and lower tip of the scapula stick out from the rib cage and become visually prominent.
.
Tension in this muscle can also cause it to compress (entrap) the nerves of the brachial plexus in the shoulder region, where the neurovascular bundle passes between the tendon of pec minor and the coracoid process of the scapula, producing neurogenic pain and numbness that is experienced in the forearm, hand, and fingers, like that associated with carpal tunnel syndrome. It may also restrict blood flow to arm by compressing the axillary artery and lead to a weak or absent pulse at the wrist of the affected arm. Because of these entrapments, trigger point activity in this muscle can be a major contributor to thoracic outlet syndrome (along with scalene trigger points).
.
Pec minor trigger points can lead to pain patterns start in the front of shoulder and can extend down the inside of the arm, elbow, forearm, palm of the hand, and into the pinky, ring, and middle fingers.
.
On the picture you can see several myofascial release techniques for the pectoralis minor muscle.
.
#Physiotherapy #Osteopathy #Injury#Prevention #Physiotherapist #Osteopath#PhysicalTherapy #Sportsmedicine#Sportstherapy #Sportsrehab #Chiropractic#Fisioterapia #Osteopatia #Fisioterapeuta#Blackroll #Pain #Fitness #Stability #Yoga#Pilates #CrossFit #Gym #Running#Stretching #Medical #Training #Muscle#Physio #Fisio #Massage
https://www.instagram.com/p/BUQrqH7A-Uq/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 5/9: PECTORALIS MINOR SYNDROME SELF-TREATMENT
As a follow up to my previous post about the PECTORALIS MINOR SYNDROME I wanted to show how you can perform a self-treatment to release tension in the pec minor muscle.
To perform this soft-tissue release:
1 Grab a Blackroll® BALL, Lacrosse ball, Tennisball, Baseball or Billiard ball.
2 Find a wall you can lean on and be able to reach one arm in front of you.
3 Place the ball on the pec minor and lean into the ball on the wall.
4 In the left video you reach your arm down at about a 45° angle and feel like you pick something off the ground, then drive your elbow up and back.
5 In the right video you perform an internal and external rotation in the shoulder joint.
https://www.instagram.com/p/BURyIjHAg6B/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 6/9: COSTOCLAVICULAR SYNDROME
The costoclavicular passage is one of three passages that consitute the thoracic outlet. The costo-clavicular passage is formed by the clavicle antero-laterally, the first rib medially, and the scapula posteriorly. The brachial nerve plexus, subclavian artery and subclavian vein run within the costoclavicular space between the first rib and the clavicle. The neurovascular bundle is vulnerable to compression in this space.
This can occur in different ways:
1 The clavicle depresses toward/against the first rib. This can be observed in the common postural condition of rounding and slumping of the shoulders. This narrows the costoclavicular passage by pushing the scapula forwards. A tight subclavius can also cause this to occur.
2 A similar mechanism operates in usually obese, middle aged or elderly women. Tight, narrow brassiere straps supporting heavy breasts cut into the soft tissues around the shoulders and exert direct downward pressure on the clavicles, usually around the junction of the mid and lateral thirds. A scissoring action of the clavicle against the first rib narrows the costoclavicular passage and shears the neurovascular bundle.
3 The first rib elevates toward/against the clavicle. This often occurs in clients who have laboured breathing. Tight anterior and middle scalenes and subclavius can also cause this to occur. The clavicle depresses and the first rib elevates.
Symptoms:
- Pain or ache sometimes accompanied by stiffness in the neck and shoulders, pain, paraesthesiae, and fatigueability of the upper limbs are the main presenting complaints.
- Symptoms are usually bi-lateral, though more pronounced on the dominant side.
- They are aggravated by work and exercise, particularly carrying heavy shopping bags.
- Symptoms are relieved by rest and sleep, are minimal or absent in the morning, and become pronounced as the day progresses.
- Patients occasionally complain of puffy blue hands.
On the picture you can see several myofascial release techniques for the scalene muscles and the subclavius muscle as well as a manual mobilization of the first rib and thoracic spine.
https://www.instagram.com/p/BUTOAOeA-xQ/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 7/9: COSTOCLAVICULAR SYNDROME
Referring to my previous post where I showed how to mobilize the structures which hold the first rib in wrong position, I wanted to show how I perform an osteopathic manipulation (chiropractic adjustment) of the first rib.
A blocked or subluxated first rib requires a mobilization. First of all you should make sure to have released all myofascial structures which cause a elevated first rib as I explained in my previous post about the 'COSTOCLAVICULAR SYNDROME'. Usually if you do a proper myofascial release treatment the first rib will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique (Osteopathic Manipulation) to get the joint to the right position otherwise it can force Thoracic Outlet Syndrome, thoracic spine, cervical spine or shoulder problems.
The video shows how I manipulate a blocked first rib, we will assume a restriction of the right first rib. With the patient in prone position the therapist stands at the top of the patients head. The therapist moves the head of the patient in cervical spine extension and turns the head with his left hand to the left side (cervical spine rotation to the right). With his right thenar placed on the rightt first rib, the therapist now performs a high velocity low amplitude (HVLA) thrust towards the table.
https://www.instagram.com/p/BUUd5oBgU6J/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 8/9: COSTOCLAVICULAR SYNDROME - OSTEOPATHIC DISTRACTION MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE CERVICO-THORACIC-JUNCTION HVLA
The C7-T1 spinal segment, also referred to as the cervico-thoracic-junction (CT Junction), is located at the very bottom of the neck.
More specifically, this is where the neck (cervical spine) connects with the upper back (thoracic spine).
Referring to my previous post a blocked first rib can force a CT Junction subluxation which requires a distraction mobilization. Even in this case you should make sure to have released all myofascial structures which are connected to the CT Junction (Trap muscle, Rhomboids, Serratus posterior superior, Erector spinae and Intrinsic back muscles).
Usually if you do a proper myofascial release treatment the CT Junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position ![]() ⚖️otherwise it can force thoracic, cervical or shoulder problems and even headaches through an so-called ascending kinematic chain.
⚖️otherwise it can force thoracic, cervical or shoulder problems and even headaches through an so-called ascending kinematic chain.
The patient is seated, almost the same hight then the therapist. The patient places his hands behind the neck and then the therapist wheels through the space in front of the shoulders and applies a distraction force!
https://www.instagram.com/p/BUV6yQlApGF/?taken-by=stefanduell
THORACIC OUTLET SYNDROME SERIES 9/9: COSTOCLAVICULAR SYNDROME - DYNAMIC TAPE TO SUPPORT THE SHOULDER GIRDLE:
This technique can help if you suffer from TOS - Costoclavicular Syndrome
Dynamic Tape to bring the shoulder complex to the right position. This technique enables to stimulate a shoulder retraction and shoulder joint external rotation to stable the whole complex and even prevent injuries such as Impingement Syndrome. The shoulder complex consists of Glenohumeral joint, Acromioclavicular joint, Sternoclavicular joint, Scapulothoracal joint and Subacromial-subdeltoid bursa.
The advantage of Dynamic Taping compare to Kinesio Taping is:
The recoil force and resistance of Dynamic Taping is many times higher then from Kinesio Taping, the focus is on creating a mechanical effect to absorb load or to resist/decelerate movement in one way or another.
With this technique and particularly if we extend it well off the scapula we can resist thoracic flexion and downward rotation of the scapula (which will also improve the length-tension relationship of the lower trapezius, which will be maintained in a more mid range position and therefore able to contract more efficiently, resist internal rotation of the humerus and anterior translation of the humeral head and provide a superiorly directed force to take the weight of the arm which may improve the length-tension of the cuff and all of which can reduce load on several structures and reduce the work requirements of the weak, fatigued or overworked muscles.
This technique is an incredible tool and supports my work a lot, especially with professional tennis players!
16. May 2017
LOW BACK PAIN SELF TREATMENT SERIES 1/7: 3 MUSCLES TO FOCUS ON
There are 3 muscles which from my own treatment experience you should always keep in mind and work on if you suffer from back and leg pain: the QUADRATUS LUMBORUM (QL), the GLUTEUS MEDIUS and the ILIOPSOAS !
The QL is a low back stabilizer, helps to depress your ribs during exhalation, and acts to laterally flex and extend the lumbar spine.
The GLUTEUS MEDIUS stabilizes the pelvis when you walk or run and abducts the leg away from the body.
The ILIOPSOAS (HIP FLEXOR) has a vital role in everyday activities like walking and running. It connects the spine to the lower extremity. It functions as a powerful hip flexor and a stabiliser of the spine and trunk during other movements. It has an important role with breathing as it attaches to the diaphragm and therefore gets affected during emotional and physical stress. Psoas is also known as the muscle of fear… Prolonged stress means a contracted or tight posas muscle!
When these muscles become tight or sensitive, they can cause intense back, pelvic, hip or leg pain, postural problems, breathing problems and stress related aches/pain. The pain you will usually feel where your glutes meet your low back at the top of your pelvis, but when bad enough, it can refer down the leg similar like sciatica.
The Iliopsoas and QL muscles are generally tight on most people in our sitting society. Both will compress the spine when they become tight! If both are on one side tighter than on the other it will compress on the same side of the spine and damaging the joints on that side + squeezing the disc to the opposite direction.
https://www.instagram.com/p/BT__Ieagx_Z/?taken-by=
LOW BACK PAIN SELF TREATMENT SERIES 2/7: GLUTEUS MEDIUS MUSCLE SELF-RELEASE TECHNIQUE
The glute med stabilizes the pelvis when you walk or run and abducts the leg away from the body.
Before you start treating your gluteus medius always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc, especially in case you feel pain radiating into your leg!!! Also make sure your health professional has cleared your hips and pelvis!
If these things are clear you take a @BLACKROLL® BALL, Lacrosse ball or tennis ball. Place it lateral, below the iliac crest and try the release exercise which you can see in the upper video (Adduction/Abduction of the hip).
Or you take a @BLACKROLL® and roll slowly among the muscle (lower video), trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Ensuring you roll from the origin to the insertion is a good way to target the entire length of the muscle.
https://www.instagram.com/p/BUBin6Mg_7C/?taken-by=stefanduell
LOW BACK PAIN SELF TREATMENT SERIES 3/7: GLUTEUS MEDIUS MUSCLE STRETCHING
Before you start stretching your glute med always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc, especially in case you feel pain radiating in your leg!!! Then the stretching is not for you as there is a totally different process of rehab for that!
Also make sure your health professional has cleared your hips and pelvis!
The stretching will bring the maximal effect if your health professional has freed your glute med muscle from trigger points and tightness! You can also release the trigger points by yourself with the exercise I showed you in my previous post!
The glute med is a muscle that can cause lower back pain, even radiating in your leg, from lack of stretching! It must be stretched daily, especially if you sit all day!
When doing these stretches for your tight glute med keep these things in mind:
- Don’t do anything that causes you more pain.
- Don’t “push through” any pain.
- Go into each position slow and controlled. You should be able to breath normal during the entire stretching position. (Breath deep into your stomach and therefore your thoracic diaphragm!)
- Hold these positions from 1-2 minutes at a time.
On the picture you can see a simple glute med stretching exercise in standing position. You can play around with this stretch subtly tweaking your hip angle can make you feel the stretch in the side of your oblique or the QL muscle or even the TFL + IT-Band, listen to your body and be aware of your surroundings! With this stretch you reach a huge portion of the Lateral Line (LL) described by Anatomy Trains!
https://www.instagram.com/p/BUCOAnJA0EH/?taken-by=stefanduell
LOW BACK PAIN SELF TREATMENT SERIES 4/7: QUADRATUS LUMBORUM MUSCLE SELF-RELEASE TECHNIQUE
The QL is a muscle that the average back pain sufferer needs to get checked out! It will bring you to your knees crawling on all 4 when acting up!
The QL is a low back stabilizer, helps to depress your ribs during exhalation, and acts to laterally flex and extend the lumbar spine.
Before you start treating your QL always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc!!! Also make sure your health professional has cleared your hips and pelvis!
If these things are clear you take a @BLACKROLL® BALL, Lacrosse ball or tennis ball. Place it above the posterior iliac crest, just to the side of the spine at the level of the hip and try the release exercise which you can see in the video.
You can either perform it as shown in the video, placing the ball under your QL and moving the hip alternately in flexion and extension or you roll slowly among the muscle, trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Ensuring you roll from the origin to the insertion is a good way to target the entire length of the muscle.
https://www.instagram.com/p/BUC0RbvgVKd/?taken-by=stefanduell
LOW BACK PAIN SELF TREATMENT SERIES 5/7: QUADRATUS LUMBORUM MUSCLE STRETCHING
Before you start stretching your quadratus lumborum muscle (QL) always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc, especially in case you feel pain radiating in your leg!!! Then the stretching is not for you as there is a totally different process of rehab for that!
Also make sure your health professional has cleared your hips and pelvis!
The stretching will bring the maximal effect if your health professional has freed your QL from trigger points and tightness! You can also release the trigger points by yourself with the exercise I showed you in my previous post!
The QL is a muscle that can cause lower back pain, even radiating in your leg, from lack of stretching! It must be stretched daily, especially if you sit all day!
When doing these stretches for your tight glute med keep these things in mind:
- Don’t do anything that causes you more pain.
- Don’t “push through” any pain.
- Go into each position slow and controlled. You should be able to breath normal during the entire stretching position. (Breath deep into your stomach and therefore your thoracic diaphragm!)
- Hold these positions from 1-2 minutes at a time.
https://www.instagram.com/p/BUDtYz-gIpc/?taken-by=stefanduell
LOW BACK PAIN SELF TREATMENT SERIES 6/7: ILIOPSOAS MUSCLE SELF-RELEASE TECHNIQUE
I found this iliopsoas muscle self-treatment technique invented by the stretch master MoveU check out their site for much more incredible stuff on self-treatments for the whole body!
The hip flexors are a huge issue for a majority of people in our “sitting” society. There are tons of ways to massage and stretch the hip flexors (rectus femoris and iliopsoas) and here is another one to add to your arsenal! This exercise requires that you barbarically jam a stick or barbell into your belly to massage the large psoas muscle that attaches to the front of your spine underneath your intestines.Do this for 30 seconds to 2 minutes per side. Please be careful with this exercise, consult your physician before doing this.
Put the stick, broom, barbell, golf club, hokey stick, etc about 1 inch to the side of your belly button and about 1 inch down. This muscle is extremely deep, try your best to relax as you do this! The more you tense up, the more it will hurt.
If you have back, hip, or knee pain… “releasing” the psoas muscle is almost always beneficial and may result is immediate pain relief and leveling of the pelvis. We have had 6 people this week with chronic hip or back pain that also had massive leg length differences. After releasing only their psoas muscle through the belly on one or both sides, their pelvic tilt and leg lengths evened out.
https://www.instagram.com/p/BUElsLDgaSI/?taken-by=stefanduell
LOW BACK PAIN SELF TREATMENT SERIES 7/7: ILIOPSOAS MUSCLE STRETCHING
The iliopsoas has a vital role in everyday activities like walking and running. It connects the spine to the lower extremity. It functions as a powerful hip flexor and a stabiliser of the spine and trunk during other movements. It has an important role with breathing as it attaches to the diaphragm and therefore gets affected during emotional and physical stress. Psoas is also known as the muscle of fear… Prolonged stress means a contracted or tight posas muscle!
The Iliopsoas and QL muscles are generally tight on most people in our sitting society. A tight iliopsoas and QL will compress the spine when they become tight! If both are on one side tighter than on the other it will compress on the same side of the spine and damaging the joints on that side + squeezing the disc to the opposite direction.
In the video you can see a simple and common exercise that, when combining with an active posterior pelvic tilt, will perfectly stretch the hip flexor in the front of the hip!
You can combine the stretch with a side bend to stretch some of the oblique and lower back (QL).
When doing these stretch for your tight iliopsoas keep these things in mind:
- Don’t do anything that causes you more pain.
- Don’t “push through” any pain.
- Go into each position slow and controlled. You should be able to breath normal during the entire stretching position. (Breath deep into your stomach and therefore your thoracic diaphragm!)
- Hold these positions from 1-2 minutes at a time.
https://www.instagram.com/p/BUFBVhWgjm1/?taken-by=stefanduell
15. May 2017
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 11/13: TEMPORALIS MUSCLE SELF-RELEASE TECHNIQUE
As a follow up to my previous post about the temporalis muscle and myofascial treatment I wanted to show how you can self-release this muscle.
The temporalis is a fan shaped muscle on each side of the skull. It attaches at the jaw, and is a major muscle involved in moving the temporomandibular joint. Excess tension here can be a big cause of headaches. This muscle works a lot, and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension. Address causal factors such as jaw clenching, stress etc. in order to get to the root of why this muscle may be developing too much tension.
To help relieve some tension in this region, massage this area at various spots. Use firm pressure, work slowly, and try to relax your head, jaw and face as much as possible. Spend 1-2 minutes doing this!
Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
If you suffer from headaches, or directly after any muscle release via fascial soft tissue work, it is very important to stay well hydrated. Pure water or Coconut water are the best options!
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to pain.
https://www.instagram.com/p/BT5gf1kgoPD/?taken-by=stefanduell
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 12/13: OCCIPITAL MUSCLES
There are 4 muscles involved in the suboccipital region also called 'Upper Cervical Spine':
1-Rectus capitis post. major
2-Rectus capitis post. minor
3-Obliquus capitis superior
4-Obliquus capitis inferior
These muscles are deeper than all other muscles in the back of the neck and they are very strongly connected to our eyes to give the feedback to the larger neck muscles as to where the head is positioned! The purpose of these muscles is to provide fine motor function in movements of the head.
The actions of trapezius, sternocleidomastoid and other larger muscles that move the head are refined by the relatively small suboccipital muscles. As the neck starts to flex in the lower cervical, our eyes always want to look forward, the head and upper cervical spine starts to extend, the suboccipitals shorten and hold the back of the skull to the top two vertebrae (Atlas and Axis) and lock it in place.
As I described already in my previous post, these muscles are also a common area to develop trigger points that can cause terrible headaches as you can see on the red marked zones in the picture. Approximately 50% of the neck rotation should come from the first two vertebrae. The rest of the cervical spine splits the other 50%, gradually rotating less and less as you progress from C3 to C7.
The suboccipital area is very prone to get stiff and immobile, when the upper cervical spine can't rotate properly, that motion get picked up by the lower cervical spine, which we want to be actually more stable!
On the picture you can see a myofascial release technique for the suboccipital muscles as well as a mobilization technique for the upper cervical spine to flexion.
Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
https://www.instagram.com/p/BT6R9zvgVDm/?taken-by=stefanduell
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 13/13: OCCIPITAL MUSCLE SELF-RELEASE TECHNIQUE
As a follow up to my previous post about the occipital muscle and myofascial treatment I wanted to show how you can self-release this muscles.
The suboccipital muscles are a group of muscles that are located below the occipital bone (base of the skull). These muscles attach at different angles and are responsible for subtle movements of the head and upper neck.
These muscles tend to get overly tight and develop a lot of extra tension. They are put in a shortened position a lot with positions like forward head posture, looking at screens etc.
This muscle tissue is a massive culprit for headaches, and extra tension here often refers into the base of the skull and elsewhere in the head.
Relieving tension here can be done using a Blackroll® BALL, Lacrosse ball or technique as shown in the video. 1-2 minutes will usually do the trick, focusing on each side separately.
If people targeted this area with myofascial release more, there would be way less medication use and chronic headaches. Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
The root cause must also be addressed, as this technique is more of a 'quick fix' to reduce or get rid of the headache symptoms.
If you suffer from headaches, or directly after any muscle release via fascial soft tissue work, it is very important to stay well hydrated. Pure water or Coconut water are the best options!
https://www.instagram.com/p/BT64EnrA0oY/?taken-by=stefanduell
14. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
Team #MeloKubot tournament champion:


09. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
Center Court

08. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 9/13: MASSETER MUSCLE SELF-RELEASE TECHNIQUE
As a follow up to my previous post about the masseter muscle and myofascial treatment I wanted to show how you can self-release this muscle.
The masseter muscle (originates at the zygomatic bone and inserts at the mandible) is the strongest muscle in the human body and can harbour some of the most common trigger points. It is a major muscle involved in moving the temporomandibular joint (Jaw joint muscle). Excess tension here can be a big cause of headaches. This muscle works a lot and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension.
To help relieve some tension in this region, massage this area at various spots. Use firm pressure, work slowly, and try to relax your head, jaw, and face as much as possible. Spend 1-2 minutes doing this!
Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
If you suffer from headaches, or directly after any muscle release via fascial soft tissue work, it is very important to stay well hydrated. Pure water or Coconut water are the best options!
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to pain
.https://www.instagram.com/p/BT3GDKXg50o/?taken-by=stefanduell
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 10/13: TEMPORALIS MUSCLE
The temporalis muscle originates at the temporal bone and inserts at the coronoid process of the mandible, it is a fan shaped muscle on each side of the skull. It is a major muscle involved in moving the temporomandibular joint (Jaw joint muscle). Excess tension here can be a big cause of headaches. This muscle works a lot and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension.
The temporalis muscle trigger points can lead to headache and toothache as well. The temporalis muscle is connected to the suboccipital muscles and shoulder muscles. Trigger points in the temporalis can initiate trigger points in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the temporalis you always have to focus on the cervical spine and shoulder region as well!
On the picture you can see several myofascial release techniques for the temporalis muscle.
If you suffer from headaches, or directly after any muscle release via fascial soft tissue work, it is very important to stay well hydrated. Pure water or Coconut water are the best options!
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to pain.
https://www.instagram.com/p/BT4J6HpgOvJ/?taken-by=stefanduell
07. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 1/13: TRAPEZIUS MUSCLE
The trap muscle is one of the largest superficial muscles that extend longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to the spine of the scapula. Its functions are to move the scapulae and support the arm.
The trap has three functional regions: the superior region (descending part), which supports the weight of the arm; the intermediate region (transverse part), which retracts the scapulae; and the inferior region (ascending part), which medially rotates and depresses the scapulae.
Contraction of the trap can have two effects: movement of the scapulae when the spinal origins are stable, and movement of the spine when the scapulae are stable. Its main function is to stabilize and move the scapula.
This muscle tends to develop too much tension for postural reasons, such as forward head posture (where it has to work overtime to stabilise the head and neck due to poor alignment). Other reasons include poor breathing patterns (shallow neck breathing all day), and muscle imbalances elsewhere.
Trap muscle trigger points can lead to referred pain in the shoulder, neck and head as you can see on the red marked zones in the picture. They also can initiate trigger points in the jaw joint muscles. Additionally, the muscle can cause biomechanical problems in the cervical and thoracic spine.
The trap is innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen, where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the trapezius. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly.
On the picture you can see several myofascial treatment techniques for the trap muscle incl. the Jugular foramen release.
https://www.instagram.com/p/BTv-tHsA_LK/?taken-by=stefanduell
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 2/13: TRAPEZIUS MUSCLE SELF-RELEASE EXERCISE
As a follow up to my previous post about the trap muscle and myofascial treatment I wanted to show how you can self-release the trap! This muscle has 3 functional parts:
- Descending (or superior) part: runs from the occipital bone and nuchal ligament to the lateral third of the clavicle.
- Transverse (or middle) part: originates from the spinal processes of the first to fourth thoracic vertebrae and inserts at the acromion.
- Ascending (or inferior) part: extends from the spinal processes of the fifth to twelfth thoracic vertebrae to the scapular spine.
Take a Blackroll® BALL, Lacrosse ball, Basball or Tennisball. Place it on the muscle and try the release exercises which you can see in the picture:
1-Ascending and transverse part
2-Descending part
Roll slowly among the muscle, trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Ensuring you roll from the origin to the insertion is a good way to target the entire length of the muscle.
Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
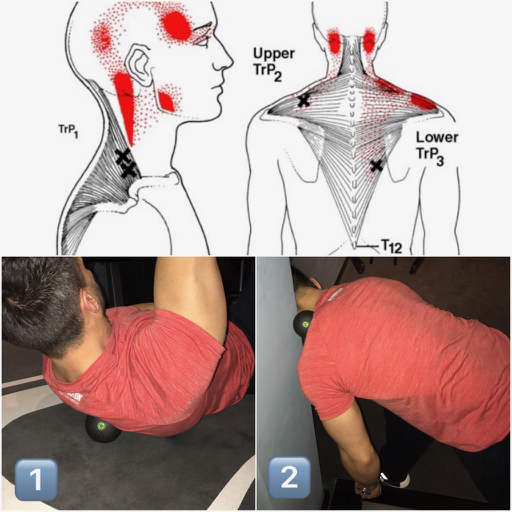
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 3/13: OSTEOPATHIC DISTRACTION MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE CERVICO-THORACIC-JUNCTION HVLA
The C7-T1 spinal segment, also referred to as the cervico-thoracic-junction (CT Junction), is located at the very bottom of the neck.
More specifically, this is where the neck (cervical spine) connects with the upper back (thoracic spine).
Referring to my previous posts the trap muscle can force a CT Junction subluxation which requires a distraction mobilization. First of all you should make sure to have released all myofascial structures which cause a CT Junction subluxation (Trap muscle, Rhomboids, Serratus posterior superior, Erector spinae and Intrinsic back muscles).
Usually if you do a proper myofascial release treatment the CT Junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems and even headaches through an so-called ascending kinematic chain.
The patient is seated, almost the same hight then the therapist. The patient places his hands behind the neck and then the therapist wheels through the space in front of the shoulders and applies a distraction force!
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 4/13: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE UPPER THORACIC SPINE SUPINE HVLA
Referring to my previous posts the trap muscle can force an upper thoracic spine subluxation which requires a mobilization. First of all you should make sure to have released all myofascial structures which cause an upper thoracic spine subluxation (Trap muscle, Rhomboids, Serratus posterior superior, Erector spinae and Intrinsic back muscles).
Usually if you do a proper myofascial release treatment the upper thoracic spine subluxation will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems and even headaches through an so-called ascending kinematic chain
We will assume a restriction at T2/3 on the left:
With the patient supine the therapist stands to the right of the patient. The patient crosses the hands behind the neck to creating stability allowing the therapist to introduce flexion to the level of dysfunction. The therapist makes a fulcrum fist with the right hand which is then placed underneath the patient with the spinous processes of T2 to T3 within. Compression is added via the therapists sternum. Through the patients flexed elbows a thrust is then delivered once the forces are focused down the line of the patients arm via the glenohumeral joint through the fulcrum hand. The force can be focused further by adding the principles of minimal leverage and enhanced by using breathing.
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 5/13: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE LOWER THORACIC SPINE SUPINE HVLA
Referring to my previous posts the trap muscle can force a lower thoracic spine subluxation which requires a mobilization. First of all you should make sure to have released all myofascial structures which cause an upper thoracic spine subluxation (Trap muscle, Serratus posterior inferior, Erector spinae and Intrinsic back muscles).
Usually if you do a proper myofascial release treatment the c-t-junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems and even headaches through an so-called ascending kinematic chain
We will assume a restriction at T9,10 on the left:
With the patient supine the therapist stands to the right of the patient. The patient crosses the elbows in front of the chest creating stability allowing the therapist to introduce flexion to the level of dysfunction. The therapist makes a fulcrum fist with the right hand which is then placed underneath the patient with the spinous processes of T9 to T10 within. Compression is added via the therapists sternum. Through the patients crossed elbows a thrust is then delivered once the forces are focused through the fulcrum hand. The force can be focused further by adding the principles of minimal leverage and enhanced by using breathing.
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 6/13: STERNOCLEIDOMASTOID MUSCLE
The sternocleidomastoid muscle (SCM) is a paired muscle in the superficial layers of the side of the neck. It is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The muscle tends to be overactive in many people we see. It is commonly recruited to help stabilise the neck/head when we adopt poor postures and positions (forward head posture). It is also an accessory muscle to breathing along with the scalenes, so having poor breathing patterns and habits will cause this muscle to overwork all day long and develop too much tension and trigger points.
The SCM trigger points can cause a variety of symptoms including headache and face pain, balance problems, visual disturbances, ear and sinus symptoms, and more body wide symptoms. They also can initiate trigger points in the jaw joint muscles. Additionally, the muscle can cause biomechanical problems in the cervical spine. It is the only muscle that creates such wide spread problems!
The SCM is innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen (a foramen in the base of the skull), where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the SCM. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly.
On the picture you can see several myofascial release techniques for the sternocleidomastoid muscle incl. the Jugular foramen release.
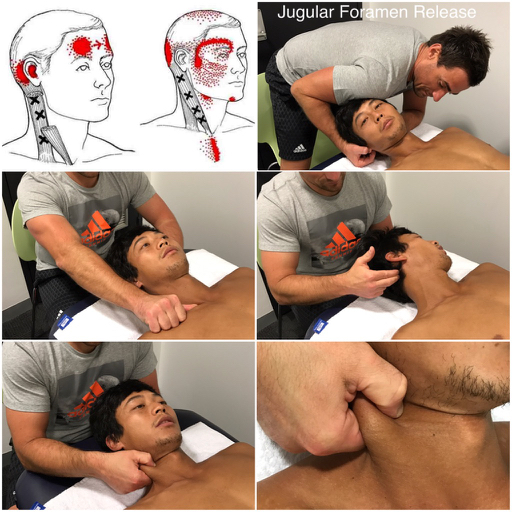
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 7/13: STERNOCLEIDOMASTOID MUSCLE SELF-RELEASE EXERCISE
As a follow up to my previous post about the sternocleidomastoid muscle (SCM) and myofascial treatment I wanted to show how you can self-release the SCM.
Excessive muscle tension in the SCM can often refer into the head and be a cause of headaches. Relieving tension can be done using a @BLACKROLL® TWISTER, Lacrosse ball, Tennisball or even your thumbs.
Especially the BLACKROLL® TWISTER is very useful as it does not only work with applying body weight to it but also allows the combination of pressure and twisting. The result: circulation rises, trigger bands and -points are stimulated and the fascial tissue becomes well hydrated:
Make sure to find the right tension areas of the SCM and apply good pressure into the muscle. Then you can twist it and move your head while the TWISTER or ball is pressed in. 1-2 minutes per side is good for the beginning!
Releasing some of this tissue can directly affect and relieve your headache without the use of any medicine!
https://www.instagram.com/p/BT1GURyAhJJ/?taken-by=stefanduell
MUSCLES WHICH CAN INITIATE NECK PAIN AND HEADACHES SERIES 8/13: MASSETER MUSCLE
.
The masseter muscle (originates at the zygomatic bone and inserts at the mandible) is the strongest muscle in the human body and can harbour some of the most common trigger points. It is a major muscle involved in moving the temporomandibular joint (Jaw joint muscle). Excess tension here can be a big cause of headaches. This muscle works a lot and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension.
.
The masseter muscle trigger points can lead to referred pain in the head as you can see on the red marked zones in the picture. The masseter muscle can force headache, toothache, tinnitus, bruxism, jaw clenching or TMJ syndrome and is connected to the suboccipital muscles + shoulder muscles. Trigger points in the masseter can initiate trigger points in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the masseter you always have to focus on the cervical spine and shoulder region as well!
.
On the picture you can see several myofascial release techniques for the masseter muscle.
.
If you suffer from headaches, or directly after any muscle release via fascial soft tissue work, it is very important to stay well hydrated. Pure water or Coconut water are the best options!
.
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to pain
https://www.instagram.com/p/BT2ASMvANEU/?taken-by=stefanduell
06. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
Just got in...

05. May 2017
Madrid - Mutua Madrid Open - ATP Masters 1000
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 5/9: STRETCHING OF THE QL
As a follow up on my QL series I wanted to show how you can stretch the QL and help yourself in case you suffer from lower back pain.
Before you start stretching your QL always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc!!! Then the stretching is not for you as there is a totally different process of rehab for that!
Also make sure your health professional has cleared your hips and pelvis first!
The stretching will bring the maximal effect if your health professional has freed your QL muscle from trigger points and tightness!
The QL is a muscle that can cause lower back pain from lack of stretching! It must be stretched daily, especially if you sit all day!
When doing these stretches for your tight QL keep these things in mind:
- Don’t do anything that causes you more pain.
- Don’t “push through” any pain.
- Go into each position slow and controlled. You should be able to breath normal during the entire stretching position.
- Hold these positions from 1-2 minutes at a time.

QUADRATUS LUMBORUM MUSCLE (QL) SERIES 6/9: OSTEOPATHIC MANIPULATION OF THE SACROILIAC JOINT USING THE CHICAGO TECHNIQUE HVLA
The QL is influencing the position of the SI-Joint. A shorten and tight QL can restrict the SI-Joint movement:
An anterior rotated Ilium bone causing a functional long leg requires posteriorization. First of all you should make sure to have released all myofascial structures which cause an anterior rotation of the ilium bone: Quadratus lumborum, Iliacus, Erector spinae, Latissimus dorsi, Adductors, Rectus femoris, Tensor fascia latae, gluteus medius and External obturator. Usually if you do a proper myofascial release treatment the ilium will correct itself but sometimes it can still stay anteriorized. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the ilium bone to the right position otherwise it can force lower back problems or even knee or foot problems!
The therapist stands on the opposite site of the dysfunction, you move the shoulders of the patient so that the upper torso is sideband away. Have the patient interlace the fingers behind the back of the neck. You now cross the leg of the opposite site over the leg nearest to you and then move the legs towards the opposite site of the table hints the patient is smiling away. This helps to focus the force at the left/right sacroiliac joint. You now insert your hand between the flexed arm of the patient that your dorsum is resting on the sternum. Introduce rotation through your arm pivoting the shoulder and the patients upper torso towards you. Place the caudal hand over the anterior superior iliac spine on the opposite site, continue rotation from above until the force is felt to accumulate under your caudal hand. Perform a high velocity low amplitude (HVLA) thrust with the caudal hand. The vector force is towards the opposite site of the table. Do not overrotate as the force will not accumulate at the sacroiliac joint!
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 7/9: OSTEOPATHIC MANIPULATION OF THE SACROILIAC JOINT USING THE LUMBAR ROLL TECHNIQUE HVLA
As a follow up to the 'Chicago Technique' to correct an anterior rotated ilium bone I wanted to show how to correct a posterior rotated ilium bone which can force tightness or trigger points in the QL!
A posterior rotated Ilium bone causing a functional short leg requires anteriorization. First of all you should make sure to have released all myofascial structures which cause an posterior rotation of the ilium bone: Hamstring muscles, Gluteus maximus muscle, Rectus abdominis muscle, Obliquus externus abdominis muscle and Adductor magnus muscle. Usually if you do a proper myofascial release treatment the ilium will correct itself but sometimes it can still stay posteriorized. If so, it requires a high velocity low amplitude (HVLA) thrusttechnique to get the ilium bone to the right position otherwise it can force lower back problems through an so-called ascending kinematic chain or even knee or foot problems through a descending kinematic chain.
For the examination of the sacro iliac junction is it important to know your anatomical landmarks! You wind down the upper body of the patient below the lumbo sacral junction plus adding flexion and rotation. This focuses the force at the superior pole of the sacro iliac joint. Using the forearm you come over the superior pole of the posterior superior iliac spine (PSIS). Now you perform a high velocity low amplitude thrust towards the therapist thereby gapping the sacro iliac joint to a neutral position.
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 8/9: OSTEOPATHIC MANIPULATION OF THE THORACO-LUMBAR-JUNCTION (TLJ) HVLA
The QL is influencing the position of the TLJ but also a blocked or subluxed TLJ is influencing the QL and can force tightness or trigger points in the QL!
A shortened and tight QL can pull the rib cage down and put an abnormal curve in your back, as if you had scoliosis, so it is very important to bring everything in balance:
The T12-L1 spinal segment, also referred to as the thoraco-lumbar-junction, is located at the very bottom of the thoracic spine.
More specifically, this is where the thoracic spine connects with the lumbar spine.
A blocked or subluxed TLJ requires a distraction mobilization. First of all you should make sure to have released all myofascial structures which cause a TLJ subluxation (Intrinsic back muscles, erector spinae, iliopsoas, quadratus lumborum, latissimus dorsi and trapezius). Usually if you do a proper myofascial release treatment the TLJ will correct itself but sometimes it can still stay in the wrong position. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems through an so-called ascending kinematic chain or lower back problems through a descending kinematic chain.
The patient stands and places his hands behind the neck and then the therapist wheels through the space in front of the shoulders and applies a distraction force via the therapists sternum through the TL Junction.
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 9/9: HOW DAILY HABITS CAN CHANGE POSTURE
If you doesn't work on biomechanical dysfunction and muscle imbalance properly it can force pain situations in your body up- or downstream through an so-called ascending or descending kinematic chain.
Consider the positions you are in throughout the day, those are your habits and your body will adapt to them! Here is a great take on this by @borisrehab:
How putting all your bodyweight on one leg can screw up your back?
I always emphasize to patients about knowing how to feel a connection with their feet to the ground (how do you ground yourself down like a sturdy) - as you can see, if you're the type of person who loves to just sag your pelvis off to one side and totally load up one leg like a crutch when standing, the long term issues can lead to all these different things happening upstream - all of a sudden 3 months later all you can complain about is this nagging back issue that seems to be an annoyance to resolve!
You keep away at the site of pain, forgetting to address and adjust and bring awareness to what the feet are doing. If your hip and your feet aren't communicating, they're not going to want to work in synchronization to create a nice stable base for your torso, chest, upper back, neck, shoulders and head to sit nicely on of. Solution? Learn to stand still. If you don't want to, then learn to play hot potato (constantly move, don't let these dysfunctional patterns solidify)!
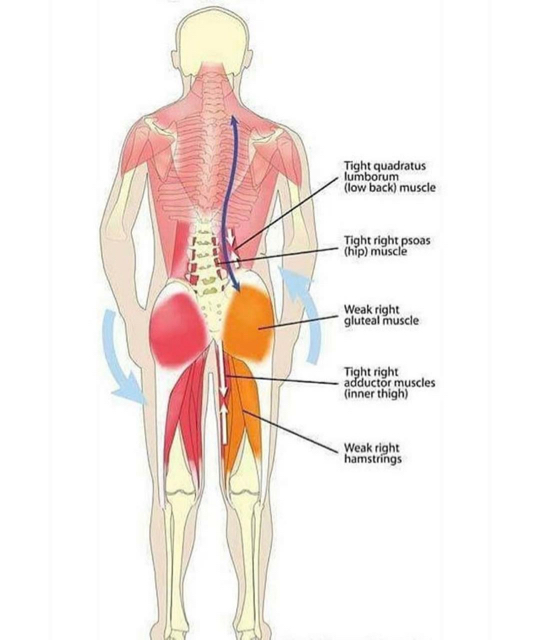
30. April 2017
Physiotherapeut Stefan Düll Sports-Physiotherapy über die folgen einseitiger Belastung beim Tennis. Lies den gesamten Artikel hier: http://www.hammer.de/…/richtig-…/bilaterales-training-tennis
29. April 2017
PIRIFORMIS MUSCLE SYNDROME (PMS) AND SELF-TREATMENT WITH THE Blackroll®
The piriformis is a small, relatively short, and little-known muscle buried deep within the muscle tissue in your hips.
In each hip, it runs from the back of your pelvis to the top of your femur. Because of its unique positioning, the piriformis muscle helps rotate your leg outward when your hip is extended, but rotates your leg inward and into abduction when your hip is flexed.
Your piriformis is positioned immediately adjacent to the sciatic nerve, a very thick nerve which runs from the base of your spine along your glute muscles and down the back of your legs, providing the nerve signals that allow all of the muscles on the back side of your lower body to fire when needed.
When the piriformis muscle is irritated, the sciatic nerve can get irritated too.
In around 15% of people, the sciatic nerve actually passes through the piriformis, which, according to some researchers, leaves these individuals more susceptible to piriformis syndrome.
Symptoms of PMS:
- Classically, it feels like an aching, soreness, or tightness in your butt, between the back of your pelvis and the top of your femur.
- Pain, tightness, tingling, weakness, or numbness can also radiate into your lower back and down the back side of your leg, through your hamstrings and calves.
- Buttock pain and tightness with prolonged sitting is also a common occurrence.
- When you run, you will probably feel pain in your butt throughout the stance phase of your stride.
Piriformis syndrome is related to sciatica, a painful irritation which also involves pain, tightness, weakness, and a numb or tingling sensation than courses down from your lower back into your butt, hamstring, and calves or even feet.
On the picture you can see diff. possibilities how to work by yourself on releasing the piriformis muscle:
1 Stretching
2 BLACKROLL®
3 BLACKROLL® BALL
#Physiotherapy #Osteopathy #Blackroll
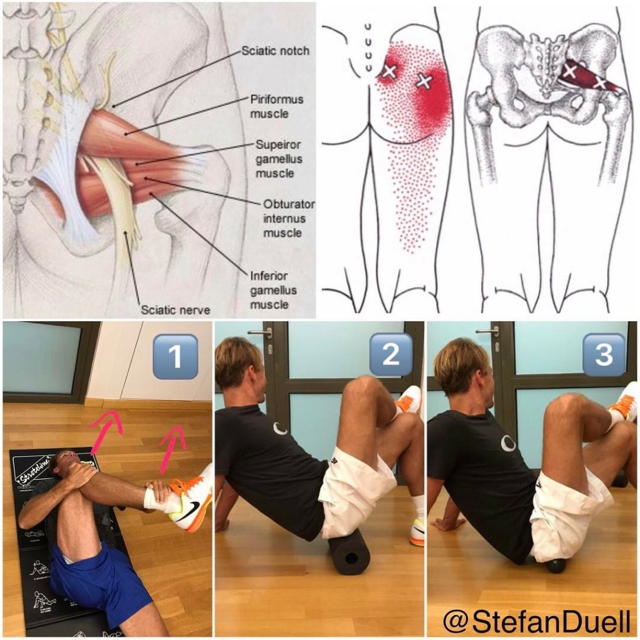
Every colleague should check this #Repost @physioosteogram
Very helpful schematic flowchart about the stomach artery and venous system especially if you work as an osteopath or therapist doing visceral manipulation work!
#Stomach #ArterySystem #VenousSystem #Visceral #Manipulation#Physiotherapy #Osteopathy
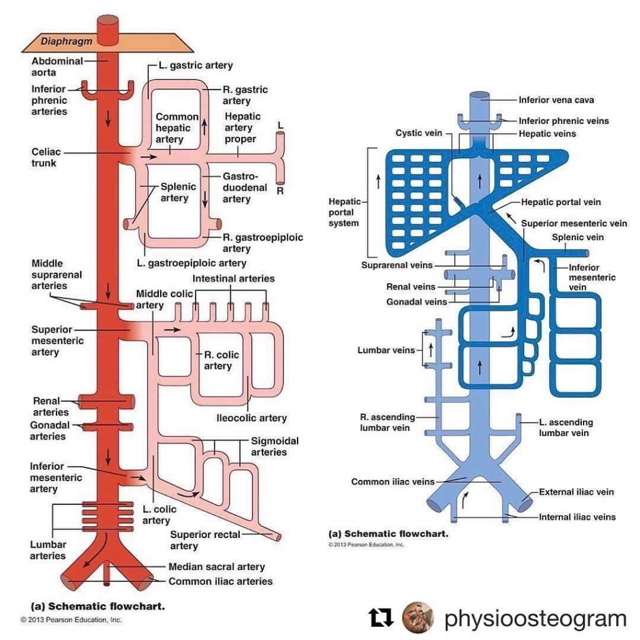
PIRIFORMIS MUSCLE AND MYOFASCIAL RELEASE TREATMET
Regarding my previous post about 'PIRIFORMIS MUSCLE SYNDROME (PMS) AND SELF-TREATMENT WITH THE BLACKROLL®' I wanted to show some myofascial treatment techniques to release the piriformis muscle and surrounding tissue manually.
Apart from the fact that the piriformis can cause an entrapment for the sciatic nerve it can also cause some biomechanical problems up- or downstream. That means if that muscle is too tight or short it can either limit the range of motion of the hip joint or it can influence the sacrum bone not being able to move in nutation properly which would have an negative effect upstream not allowing the lumbar spine to move in lordosis which can cause terrible lower back problems!
Additionally, piriformis muscle trigger points can lead to referred pain in the lower back, buttocks and down the back side of your leg, through your hamstrings as you can see on the red marked zones in the picture.
So better keep this muscle in shape! With the Blackroll® exercises I showed in my previous post you have some nice tools to do so. This work will help everyone but especially office workers who are sitting all day long!
On the picture you can see several myofascial release techniques for the piriformis muscle.
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
https://www.instagram.com/p/BTbgBNAgZ_J/?taken-by=stefanduell
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 1/8: ANATOMY AND FUNCTION
The QL will bring you to your knees crawling on all 4 when acting up! It is a muscle that the average back pain sufferer needs to get checked out to make sure it’s not the reason of your on going problems!
The quadratus lumborum muscle is a muscle of the posterior abdominal wall lying deep inside the abdomen and dorsal to the iliopsoas. In order to palpate the muscle one needs place the fingers above the posterior iliac crest at the level of the hip. Starting from the iliac crest of the ilium/iliolumbar ligament (Origin) and from there it runs craniomedially, and attaches to the 12th rib and the transverse processes of the 1st to 4th lumbar vertebrae Insertion). All fibers together give the muscle a rectangular appearance. The innervation is supplied by the subcostal nerve and branches of the lumbar plexus.
The quadratus lumborum fills a great amount of space within the abdomen and is therefore in close proximity to many structures. The colon, the kidneys and the diaphragm are located ventrally to the muscle, whereas the intrinsic back muscles lie dorsomedially. Both the iliohypogastric and ilioinguinal nerves course on the ventral surface of the quadratus lumborum after exiting the lumbar plexus and continue towards the lateral abdominal muscles.
The QL is made up of 3 sets of fibers:
Iliocostal fibers (Ilium to 12th rib)
Iliolumbar fibers (Ilium to Lumbar TVPs)
Lumbocostal fibers (Lumbar TVPS to 12th rib)
Function
Essentially, the quadratus lumborum contributes to the stabilization and movement of the spine and the pelvis.
A bilateral contraction leads to an extension of the lumbar vertebral column.
A unilateral contraction leads to the trunk is bent towards that direction (lateral flexion) and it can also hike up the same sided hip.
A contralateral contraction rotates the spine.
It can also cause functional scoliosis if the upper fibers bends one way and the opposite lower fibers bends the other way.
In addition, the muscle fixes the 12th rib during movements of the thoracic cage and this way supports expiration (accessory muscle of expiration).
How do I know if my QL is tight?
Your lower back pain over time develops into what seems like a sciatica (pain in buttocks, hips, groin and leg).
When acting up coughing or sneezing it will bring sharp agonising pain.
People constantly attempting to brace and stabilize their upper body with their hands while they stand or sit is a sure fire sign of an over firing QL.
Being in an upright or sitting posture makes the pain worse but most individuals will experience pain with any movement.
Rolling from side to side after laying face up for some time is extremely painful.
If you’re aware of one leg being genetically shorter than the other and you’re suffering from back pain you could be a good candidate for a tight QL.
In my next post i will show how to release the QL muscle, stay tuned!

QUADRATUS LUMBORUM MUSCLE (QL) SERIES 2/8: PATHOLOGY AND MYOFASCIAL TREATMENT
Overuse and strain of the quadratus lumborum are one of the major causes for chronic pain in the lower back. One typical cause is the habit of sitting at the desk using a reclined seat, which releases the intrinsic back muscles and weakens them in the long term. The weak back muscles must now be compensated by the quadratus lumborum leading to painful tension and stiffening of the muscle. Other causes can be direct damage (tightness, shortening or trigger points) or any type of imbalance of the pelvis or spine which forces the QL to stabilize them. An example of that type of imbalance is unequal leg lengths.
A shorten and tight QL can restrict pelvic movement, pull the ribcage down and put an abnormal curve in your back, making you appear to have scoliosis or a short leg.
A tight QL can be caused by a weak and inhibited Gluteal muscles. When your butt is slacking your QL is working extra hard which eventually tires out and all of a sudden you blow out your back picking up a pen off the ground. The thing is if you’re not training in a way that will repair that imbalance than simply mashing on a tight QL won’t bring you lasting relief. You have to look at the root cause.
QL trigger points can lead to referred pain in the lower back, stomach, buttocks and down of your leg as you can see on the red marked zones in the picture.
One reason that your QL may lock up is due to imbalances in your hips and pelvis. Before you start working on the QL you need to clear the hips and pelvis! For the diagnose it is very important to eliminate every single reason which could lead to hip and pelvis imbalances, that means always check the full body: feet, knees, hips, pelvis, upper body and don’t forget in this case especially the colon, the kidneys nd the diaphragm as they are located ventrally to the muscle and also can have an influence.
On the picture you can see how I approach the quadratus lumborum muscle for a myofascial release treatment:
Out of this position with your thumb you can perform 1 a trigger point technique or 2 a release technique for the fascia of the QL.
1 If you want to perform a trigger point technique make sure you hold the pressure as long the patient tells you the pain or the radiation goes down or the pain is not radiating anymore but at least for 1 minute and finish the technique then with a Ponçage. I usually hold the pressure until I feel a myofascial release under my finger!
2 If you do the complete QL fascial release technique make sure you perform the technique from origin to insertion to lengthen the fascia if the QL is shortened or from insertion to origin to shorten the fascia if the QL is lengthened!
in my next post i will show how to perform a self-treatment on the QL muscle, stay tuned!
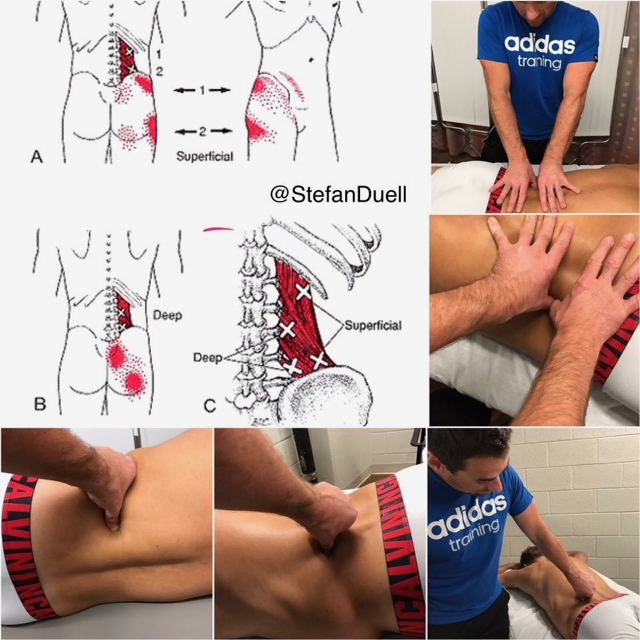
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 3/8: COLLAPSE OF THE RIB CAGE AND/OR HIP HIKE
This video is a great follow up to my QL pathology post 2 days ago. Consider the positions you are in throughout the day, those are your habits and your body will adapt to them!
Checkout the following post from @borisrehab:
'HOW SITTING IMPROPERLY CAN GIVE YOU SCOLIOSIS!?
Are you sitting down at the moment? Pay close attention to which side you lean more on. Odds are you favour one side over the other. Whichever side you prefer, will cause the opposite side of your low back (specifically the QL for you out there) to tighten! In A you can see that the person is leaning more on his right butt cheek and that causes his spine to twist into a minor functional S-shaped scoliosis.
In B if you place a book underneath that person's right buttocks he will seem to have a straighter spine.
In C, the book is placed under the left buttocks and that sends the spine into a major S-shape! So imagine if you're sitting a certain way, and you have your wallet in one of your back pockets. The wallet might be the reason you have low back pain! So not only is it important to release the left QL in this particular situation, you have to make sure you rectify what's causing it to be tight in the first place!'
https://www.instagram.com/p/BTjAMT4AjTh/?taken-by=stefanduell
QUADRATUS LUMBORUM MUSCLE (QL) SERIES 4/8: SELF-TREATMENT OF THE QL MUSCLE
Regarding my previous post about the manual myofascial treatment of the QL I wanted to show how you can self-release the QL.
Before you start treating your QL always make sure you saw a health professional first who confirmed you doesn’t suffer of a herniated disc!!! Also make sure your health professional has cleared your hips and pelvis!
If these things are clear you take a Blackroll® BALL, Lacrosse ball, Base Ball or Tennis Ball. Place it above the posterior iliac crest, just to the side of the spine at the level of the hip and try the release exercise which you can see in the video.
You can either perform it as shown in the video by @vitasphysio: placing the ball under your QL and moving the hip alternately in flexion and extension or you roll slowly among the muscle, trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Ensuring you roll from the origin to the insertion is a good way to target the entire length of the muscle.
After any muscle release via soft tissue work as shown in the first part of the video it is important to reintegrate that muscle into a movement! In the video you can see a „butt walk“ to put some fire in the QL muscle. As the two main functions of the QL are extension and side flexion of the spine, the „butt walk“ incorporates both. It is also a great drill to warm up the low back before any lifting session!
https://www.instagram.com/p/BTjh0fzAbWk/?taken-by=stefanduel
23. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
Shout out to Yen-Hsun Rendy Lu on capturing his 27th ATP World TourChallenger title in Taipei today! Must be very special in front of home crowd, family and friends! Bravo Rendy! Taiwan can be proud to have such an incredible tennis player who made history for his country!!!

21. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
THE POPLITEUS MUSCLE
The popliteus muscle is a fairly small muscle located behind the knee. It runs from the lateral side of the femur to the medial side of the tibia, lying deep beneath the main calf muscle. Its role is to unlock the knee just after the heel touches the ground when you are walking or running. It also has an important role when running downhill as it assists the posterior cruciate ligament (PCL) in decelerating the femur and preventing its sliding forward on the tibia.
Because of its role in assisting the PCL on downhills, runners can start developing symptoms after an abnormally long hill-training session. People with unstable knees (torn ligaments, torn meniscus, arthritis…) are also prone to develop a popliteus problem because of its important role in stabilizing the knee. The popliteus muscle is kind of a muscle, if there are any irritations inside or outside the knee happening the popliteus usually reacts with tightness and triggerpoints which can lead to pain situations of the knee.
Popliteus muscle problems remain under-diagnosed to this day, meaning that a lot of runners suffer from it without knowing. Its small role in gait function and its deep location make it unsuspected and underestimated by a lot of health professionals. Also its symptoms are strangely very similar to those of a torn collateral ligament, a torn meniscus or a Patellofemoral Syndrome. So if you have been experiencing knee pain and it does not seem to heal, ask your health professional about the popliteus.
Popliteus muscle problems simply appear as tendonitis, muscle tightness or triggerpoints so it should be treated the same way meaning anti-inflammatory and physio treatment. Especially with fascial and triggerpoint treatments I experienced very good results! Popliteus muscle problems are fairly easy to treat and respond well to treatment, but the challenge remains in the diagnosis… so keep your eyes open!
On the picture you can see several myofascial treatment techniques for the popliteus muscle and its fascia.

THE SPLENIUS-RHOMBOID-SERRATUS ANTERIOR SLING
Did you know that the splenii muscles (splenius capitis and splenius cervicis), the rhomboid muscles (rhomboid major and rhomboid minor) and the serratus anterior muscle are actually connected!?
On the picture you can see a very important connection of fascial tissue: THE SPLENIUS-RHOMBOIDEUS-SERRATUS ANTERIOR SLING by Anatomy Trains
That means, if you have problems/tightness in your cervical spine, your shoulder will be equally affected on the opposite site!
If you suffer from cervical/thoracic spine or shoulder problems, always make sure that your therapist is checking not only one area. The root of shoulder pain is almost always not only in the shoulder!
Picture credit: Anatomy Trains
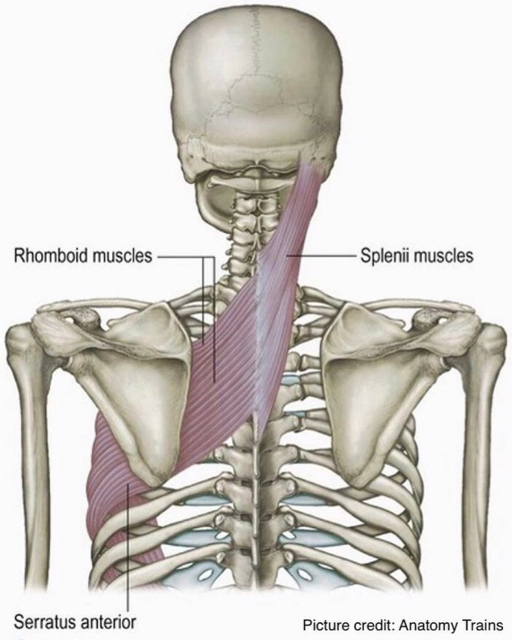
This demonstration fits exactly to my previous post about the SPLENIUS-RHOMBOID-SERRATUS ANTERIOR SLING, because this sling is actually a part of the SPIRAL LINE by Anatomy Trains!
https://www.instagram.com/p/BTUiG6sAuN4/?taken-by=stefanduell
THE INTERACTION OF LATISSIMUS DORSI MUSCLE, TERES MAJOR MUSCLE AND PECTORALIS MAJOR MUSCLE
Did you know that the latissimus dorsi muscle, the teres major muscle and the pectorals major muscle are actually connected!?
On the picture you can see all 3 muscles which belong to the same fascial connection: THE SUPERFICIAL FRONT ARM LINE (SFAL) by Anatomy Trains.
If you suffer from neck or shoulder problems (rounded shoulders) always make sure to treat these muscles in the right way!
Latissimus dorsi, teres major and pectoralis major are medial rotators of the humerus, that means that if you overtrain these structures, it will force rounded shoulders!
I am specifically mentioning this because of how many people you see in the gym doing bench press and lat pulldown all training session long without doing any stretching or exercises to keep the shoulder girdle in balance!
Even if you don't suffer from any problems or pain right now, but you train in the wrong way over a period of time you can train yourself into a misalignment which will lead to shoulder, cervical/thoracic spine problems, tension in upper traps or headaches!
Especially for those who spend the majority of their day sitting, such as office workers or those who spend the majority of their day in a hunched position such as dentists, it is very important not to overtrain these structures. Being in a poor position and using this muscles will cause an adaptive shortening and tightness already!
Important for therapists is to release and lengthen these muscles if your patient is suffering from rounded shoulders!
Picture credit: Anatomy Trains
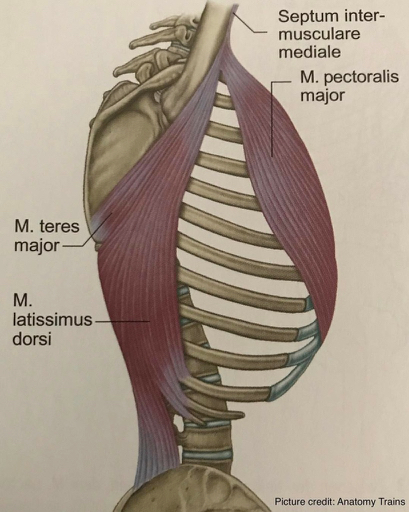
SUPERFICIAL FRONT ARM LINE (SFAL)
To everybody who is critical with my previous post about the connection of latissimus dorsi muscle and pectoralis major muscle: here is a picture with a preparation of the full SUPERFICIAL FRONT ARM LINE (SFAL) by Anatomy Trains.
Thomas Myers, the founder of Anatomy Trains did his own dissections on untreated, fresh-tissue cadavers to proof his theoretical thinking!
You can see exactly that the latissimus dorsi muscle and the pectoralis major muscle join in the medial intermuscular septum of the arm which is further connected to the forearm flexor muscles and the palmaris longus muscle including the carpal tunnel.
Thank you to Thomas Myers for this incredible work!
Picture credit: Anatomy Trains
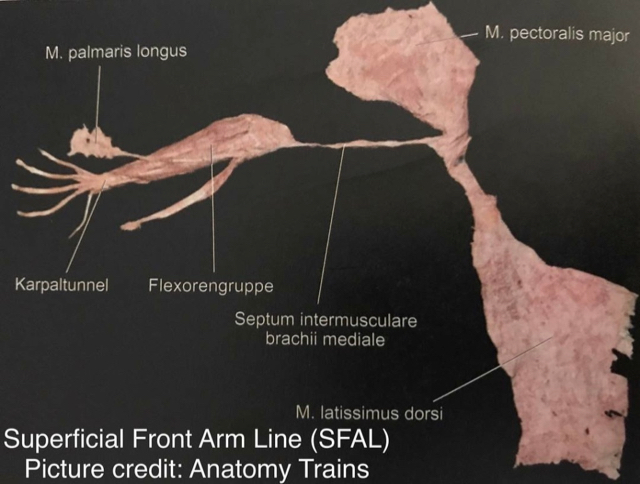
This demonstration fits exactly to my previous post talking about the connection of 'LATISSIMUS DORSI MUSCLE AND PECTORALIS MAJOR MUSCLE', you can see in 3-D version how they attach/connect at the humerus bone. Both are part of the Anatomy Trains SUPERFICIAL FRONT ARM LINE.
https://www.instagram.com/p/BTYSG2EgCcR/?taken-by=stefanduell
20. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
MYOFASCIAL RELEASE OF THE SUBOCCIPITAL MUSCLES AND OSTEOPATHIC MANIPULATION OF THE OAA COMPLEX HVLA
There are 4 muscles involved in the suboccipital region also called 'Upper Cervical Spine': Rectus capitis posterior minor, Rectus capitis posterior major, Obliquus capitis inferior and Obliquus capitus superior. These muscles are deeper than all other muscles in the back of the neck and they are very strongly connected to our eyes to give the feedback to the larger neck muscles as to where the head is positioned!
The purpose of these muscles is to provide fine motor function in movements of the head. The actions of trapezius, sternocleidomastoid and other larger muscles that move the head are refined by the relatively small suboccipital muscles. As the neck starts to flex in the lower cervical, our eyes always want to look forward, the head and upper cervical spine starts to extend, the suboccipitals shorten and hold the back of the skull to the top two vertebrae (Atlas and Axis) and lock it in place. These muscles are also a common area to develop trigger points that can cause terrible headaches.
Approximately 50% of the neck rotation should come from the first two vertebrae. The rest of the cervical spine splits the other 50%, gradually rotating less and less as you progress from C3 to C7.
The suboccipital area is very prone to get stiff and immobile, when the upper cervical spine can't rotate properly, that motion get picked up by the lower cervical spine, which we want to be actually more stable!
On the picture you can see several myofascial release techniques for the suboccipital muscles as well as a mobilization technique for the upper cervical spine to flexion and an Osteopathic Manipulation of the Occiput-Atlas-Axis (OAA) Complex using the Chin-Hold-Technique HVLA. Usually if you do a proper myofascial release treatment, the OAA Complex will get into the right position by itself. If not, it requires a high velocity low amplitude (HVLA) thrust technique! In this case the Atlas had a shift lesion to the right.

MYOFASCIAL RELEASE OF THE TRAPEZIUS AND STERNOCLEIDOMASTOID MUSCLE (SCM)
The trapezius muscle is one of the largest superficial muscles that extend longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to the spine of the scapula. Its functions are to move the scapulae and support the arm.
The trapezius has three functional regions: the superior region (descending part), which supports the weight of the arm; the intermediate region (transverse part), which retracts the scapulae; and the inferior region (ascending part), which medially rotates and depresses the scapulae. Its main function is to stabilize and move the scapula.
The trapezius muscle trigger points can lead to referred pain in the shoulder region and head as you can see on the red marked zones in the picture. Additionally, the muscle can cause biomechanical problems in the cervical and thoracic spine.
The sternocleidomastoid muscle (SCM) is a paired muscle in the superficial layers of the side of the neck. It is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The SCM trigger points can cause a variety of symptoms including head and face pain, balance problems, visual disturbances, ear and sinus symptoms, and more body wide symptoms. It is the only muscle that creates such wide spread problems. Trapezius muscle and SCM trigger points can initiate trigger points in the jaw joint muscles.
Both muscles are innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen (a foramen in the base of the skull), where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the trapezius and SCM. That's why it is very important to release this foramen to give the nerve enough space to work properly.
On the picture, you can see the jugular foramen release technique as well as several myofascial release techniques for both muscles.
(Treatment strategy and techniques by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
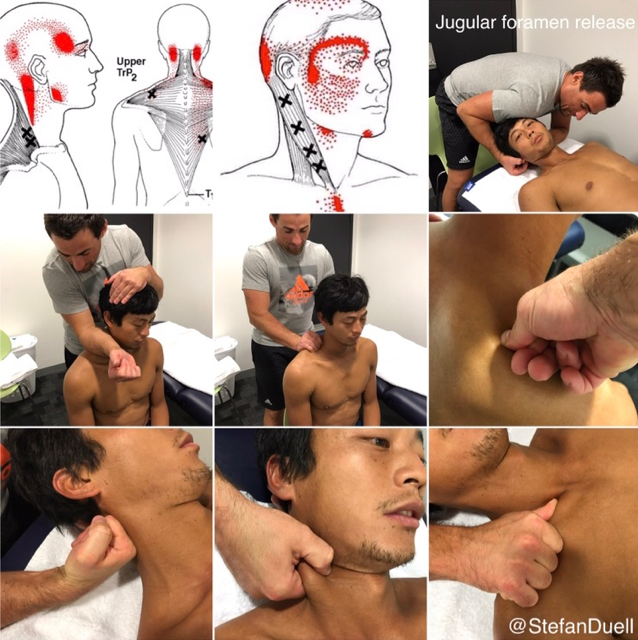
MYOFASCIAL RELEASE OF THE LONGUS COLLI/CAPITIS MUSCLE
The longus colli gets its name for the Latin for long muscle of the neck. The muscle acts as a flexor of the head and neck when its acts bilaterally, and causes rotation to the ipsilateral side when it acts unilaterally. The longus colli consists of three sections: a superior oblique, an inferior oblique and a vertical. The arterial supply to the muscle comes from the muscular branches of the ascending cervical artery. The innervation to the muscle comes from the anterior rami of the 2nd to 6th cervical spinal nerves.
Despite its importance, the longus colli isn’t well known or appreciated which is very unfortunate, as in my experience it is a very important muscle to have always in focus, especially if your patient is suffering from cervical spine problems!
Once you understand its position and actions, it is not surprising that the longus colli can be a source of neck pain. Not only because it is sore or hurt, but because when it gets too tight it can force a cervical spine kyphosis or straight neck (Military Neck). This happens very often after suffering from a whiplash injury.
The longus colli muscle trigger points can lead to referred pain in the neck and ear as you can see on the red marked zones in the picture. Additionally, it can cause tinnitus, a sore throat, painful speech, thyroid gland disturbance and functional disturbance of the heart.
On the picture you can see how i approach the longus colli muscle for a myofascial trigger point treatment. Make sure you hold the pressure as long the patient tells you the pain or the radiation goes down or the pain is not radiating anymore but at least for 1 minute and finish the technique then with a Ponçage. I usually hold the pressure until i feel a myofascial release under my finger!
(Treatment technique by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
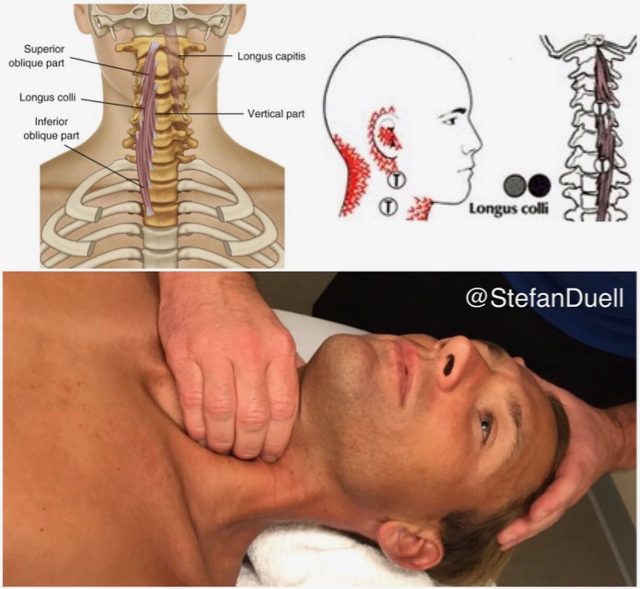
19. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
SHOULDER PAIN SERIES 23/23 - FUNCTIONAL STABILITY EXERCISE FOR THE SHOULDER JOINT:
Just got introduced to a new training device, called The Yoak which is very helpful if you want to work on proprioceptive training to stabilize the shoulder girdle and joint, especially for over head sports -> HIGH END SHOULDER STABILITY!
Yoak Get-Up/Windmill Combo
Using 'The Yoak' for that type of injury resistance training for the shoulder is my go to!
Try this variation to change things up if you typically only go overhead with military presses or Olympic lifts. The time under tension in the overhead position along with the added stability challenge can really bullet proof those shoulders to injury.
- Start light. Time under tension and instability of the load is what makes this challenging. Go heavy with your foundational lifts, not this supplemental work.
- For a different challenge, instead of the windmill/get up combo, do the get up/overhead carry combo.
For video click here:
https://www.instagram.com/p/BTI4GEkAaGG/?taken-by=stefanduell
18. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
SHOULDER PAIN SERIES 21/23 - SCAPULAR STABILITY - SCAPULAR AND CORE CONTROL:
Now that you've worked on different stabilizing muscles of the scapula in the previous posts let's work on more advanced functional exercises to prepare the scapulothoracal joint for tougher situations in daily life or your overhead sport -> HIGH END SCAPULAR STABILITY!
The exercise shown in the video requires a lot of scapular and core control!
Being able to move slowly under control is the key to this for any given movement, make sure you can do it slowly. You need to dictate the movement and be in control the entire time. Choose random exercises every once in a while that are outside of your usual routine!
Activate your CORE muscles before you start the exercise as I explained in my previous post about `STRENGTHENING THE CORE MUSCLES`.
Do the movements slow and controlled and work up to 3 sets of 5-10.
For video click here:
https://www.instagram.com/p/BTEAFzUAOiN/?taken-by=stefanduell
SHOULDER PAIN SERIES 22/23 - SHOULDER GIRDLE STABILITY - SHOULDER BLADE ADDUCTION AND SHOULDER JOINT EXTERNAL ROTATION EXERCISE:
Now that you've worked on scapular stability in the previous posts let's work on some exercises for the rotator cuff of the shoulder joint to give the shoulder girdle even more stability and being ready for the competition!
Crossover Symmetry training to protect the shoulder joint is very important and a basic part of an injury prevention or rehab program. This video shows a combined shoulder blade adduction and external rotation exercise which is very important to keep the shoulder girdle in the right position. Essential for all athletes especially professional tennis players to keep them free of pain and injuries in the shoulder joint!
Quick anatomy review:
The external rotators of the shoulder are:
- Infraspinatus
- Teres Minor
- Posterior Deltoid
Personally, I like doing this workout with the Crossover Symmetry device as in the video or a TheraBand but it can also be done with Dumbbells too!
Activate your CORE muscles before you start the exercise as I explained in my previous post about `STRENGTHENING THE CORE MUSCLES`.
Do the movements slow and controlled and work up to 3 sets of 15.
17. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
SHOULDER PAIN SERIES 20/23 - SCAPULAR STABILITY - TRAPEZIUS MUSCLE (ASCENDING PART) ACTIVATION:
Now that you've worked on your serratus anterior muscle, rhomboids and mid traps in the previous posts let's work on another very important structure to create even more control in the scapulothoracic joint, the ascending part of the trapezius muscle.
The video shows how to train and put some load into the lower part of the trapezius muscle (ascending part) which is essential for a good posture and therefore a well functioning cervical spine, shoulder joint and upper limb. It is very often forgotten in the conventional workouts to work on this particular movement. This exercise is designed not only for professional athletes - it´s very important for everyone to include it into your training routine especially if you suffer from cervical spine or shoulder problems!
Do the movements slow and controlled and work up to 3 sets of 15.
Check my previous posts about the trapezius muscle and it's relation to the pectoralis minor muscle to understand better why it is so important to put some into the ascending part of the trapezius muscle especially if you suffer from rounded shoulders!
16. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
SHOULDER PAIN SERIES 19/23 - SCAPULAR STABILITY - RHOMBOIDS + MIDDLE TRAPS MUSCLE ACTIVATION:
In this video you can see another possibility to target the rhomboids and middle traps to get them firing!
I actually prefer this exercise compared to the one I posted yesterday, but the yesterday's one might be easier for beginners to get used to the movement!
You are in a laying position and use any kind of sling training device (TRX Training) with your arms outstretched and elbows slightly bent. Make sure the movement happens in the shoulder girdle by retracting your scapula back towards your spine leaving your arms as they started.
Activate your CORE muscles before you start the exercise as I explained in my previous post about `STRENGTHENING THE CORE MUSCLES.
Do the movements slow and controlled and work up to 3 sets of 15.
15. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
SHOULDER PAIN SERIES 18/23 - SCAPULAR STABILITY - RHOMBOIDS + MIDDLE TRAPS MUSCLE ACTIVATION:
Now that you've worked on your serratus anterior muscle in the previous post let's work on the rhomboids and middle traps to create some more control in the scapulothoracic joint.
I have chosen to show this exercise at this place because the rhomboids are intimately connected to the serratus anterior muscle and makes a sling for the scapula to balance between protraction and retraction!
Rowing is a very good exercise to target on the rhomboids and middle traps but you need to perform it with a modification to get the rhomboids and traps firing !
You can use a rowing cable machine or a Thera Band.
Stand or sit in an upright position with your arms outstretched and elbows slightly bent. Make sure the movement happens in the shoulder girdle by retracting your scapula back towards your spine leaving your arms as they started.
Activate your CORE muscles before you start the exercise as I explained in my previous post about `STRENGTHENING THE CORE MUSCLES.
Do the movements slow and controlled and work up to 3 sets of 15.
14. April 2017
Monte Carlo/Monaco - Monte Carlo Rolex Masters - ATP 1000
Just checked in at this amazing place: Monte-Carlo Rolex Masters (Official). Definitely one of the most beautiful tennis clubs in the world! #MonteCarloCountryClub

SHOULDER PAIN SERIES 17/23 - SCAPULAR STABILITY - SERRATUS MUSCLE ACTIVATION:
Scapula winging is a surprisingly common physical sign, but because it is often asymptomatic it receives little attention. What happens when we let that scapula wing? We lose serratus anterior muscle function, some lower trap function and all of the shoulder stabilizers are weakened.
What causes this if it isn't from an injury? Always being in a state of poor posture (office workers, dentists) or just simply not hitting the right muscles during your training. Often overworking your pecs and upper traps can add to the problem, if you are not spending enough time working the muscles that act on the scapula itself. It goes without saying, if you have serious pain, or loss of function in the upper back and shoulder area, go see your doc first.
How do you fix it? Strengthening up your serratus anterior is a great place to start!
In the video you can see a serratus anterior exercise on all fours (quadruped), also called Scapular Push-ups (Pro-/Retraction of the Scapula).
Beginner Version with knees on the floor and Advanced Version with knees lifted from the floor.
Activate your CORE muscles before you start the exercise as I explained in my previous post about 'STRENGTHENING THE CORE MUSCLES'.
Do the movements slow and controlled and work up to 3 sets of 15.
Another very good possibility to train the serratus anterior is getting patients to practice crawling on the ground as not only does it get your serratus anterior firing well but it is also a fundamental human movement that helps restore stability to the shoulder complex!
12. April 2017
Würzburg
SHOULDER PAIN SERIES 15/23 - THE FASCIAL DISTORTION MODEL™:
Fascial Distortion Model™ (FDM) developed by Dr. Stephen Typaldos D.O., a very good and effective therapy method not only if you work with professional athletes. I experienced incredible good results with that method!
What is FDM?
FDM is a model of diagnosis and treatment for common musculoskeletal conditions. FDM practitioners can diagnose and treat virtually every musculoskeletal injury. Using six specific problems (or “distortions”) in the body’s connective tissue, we can improve conditions such as pulled muscles, strains, sprains, and frozen shoulders. So why use FDM? Patients can benefit from a quicker reduction in pain, and often immediate improvements in movement restrictions.
The distortions:
FDM describes six different distortions (Triggerband, Folding Distortion, Continuum Distortion, Herniated Trigger Point, Cylinder Distortion and Tectonic Fixation) which are commonly shown through a person’s body language or hand signals. The FDM practitioner listens to and watches the patient to diagnose these distortions. The practitioner then follows up with treatments specific to the patient’s description of his/her pain.
After the treatment it is very important to move, as excessive resting does not give your body´s tissue a chance to heal correctly! You also can apply ice to areas treated or sore. Do NOT apply ice directly on skin; cover with a paper towel or towel. Apply 5 min only and repeat often (5-10 times within 24 hrs of your treatment session). If heat is something you love to do, then wait 48 hrs after treatment.
On the picture you can see how I start to treat a 'Ventral Shoulder Triggerband'. Triggerbands are the most common distortions of all, triggerbands are twisted or wrinkled fascial fibers that cause a burning or pulling pain along fascial structures that are comprised primarily of linear fibers (such as fascial bands, ligaments, and tendons). When verbally describing their discomfort, athletes and other patients with triggerband injuries subconsciously make a sweeping motion with their fingers along the anatomical course of the injured fascial fibers.
In Germany you can attend the course at Deutsches Fortbildungsinstitut für Osteopathie or Infomed!

SHOULDER PAIN SERIES 16/23 - DYNAMIC TAPE TO SUPPORT THE SHOULDER JOINT:
This technique can help if you suffer from shoulder problems:
Dynamic Tape to bring the shoulder complex to the right position. This technique enables to stimulate a shoulder retraction and shoulder joint external rotation to stable the whole complex and even prevent injuries such as Impingement Syndrome. The shoulder complex consists of Glenohumeral joint, Acromioclavicular joint, Sternoclavicular joint, Scapulothoracal joint and Subacromial-subdeltoid bursa. The advantage of Dynamic Taping compare to Kinesio Taping is: The recoil force and resistance of Dynamic Taping is many times higher then from Kinesio Taping, the focus is on creating a mechanical effect to absorb load or to resist/decelerate movement in one way or another. With this technique and particularly if we extend it well off the scapula we can resist thoracic flexion and downward rotation of the scapula (which will also improve the length-tension relationship of the lower trapezius, which will be maintained in a more mid range position and therefore able to contract more efficiently, resist internal rotation of the humerus and anterior translation of the humeral head and provide a superiorly directed force to take the weight of the arm which may improve the length-tension of the cuff and all of which can reduce load on several structures and reduce the work requirements of the weak, fatigued or overworked muscles.
This technique is an incredible tool and supports my work a lot, especially with professional tennis players!
11. April 2017
Würzburg
SHOULDER PAIN SERIES 12/23 - PROTRACTED SHOULDER GIRDLE - MYOFASCIAL RELEASE OF THE SUBCLAVIUS MUSCLE:
The subclavius muscle is a short muscle of the shoulder girdle. It originates at the first rib (border between the bone and cartilage) and inserts at the lower surface of the lateral clavicle. The main task of the subclavius muscle is the active stabilization of the clavicle in the sternoclavicular joint during movements of the shoulder and arm. Furthermore its contraction leads to a depression of the clavicle and elevation of the first rib respectively. .
Its importance lies in the fact that it can influence the movement and position of the shoulder joint.
Despite its importance, the subclavius isn’t well known or appreciated which is very unfortunate, as in my experience it is a very important key muscle to have always in focus, especially if your patient is suffering from shoulder or cervical spine problems!
Once you understand its position and actions, it is not surprising that the subclavius can be a source of shoulder pain, not only because it is sore or hurt, but because when it gets too tight it can pull the shoulder forward and down, thus misaligning the shoulder joint. Any time the gleno-humeral joint, sterno-clavicular joint or acromio-clavicular joint aren't aligned properly, pain can arise. The subclavius muscle triggerpoint can lead to referred pain in the arm as you can see on the red marked zones in the picture. Additionally, the muscle can cause biomechanical problems in the cervical spine, due to its influence on the first rib in terms of elevating it, as the rotation in the cervical spine will be irritated.
On the picture you can see different possibilities of treating the subclavius muscle.

SHOULDER PAIN SERIES 13/23 - THE LATISSIMUS DORSI MUSCLE:
The latissimus dorsi muscle, whose name means “broadest muscle of the back,” is one of the widest muscles in the human body. Also known as the “lat,” it is a very thin triangular muscle that is not used strenuously in common daily activities but is an important muscle in many exercises such as pull-ups, chin-ups and lat pulldowns.
The latissimus dorsi muscle has its origins along the lumbodorsal fascia of the lower back, arising from the inferior thoracic and lumbar vertebrae, sacrum, iliac crest, and the four most inferior ribs. From its many widespread origins, it runs obliquely, superiorly and laterally through the back and armpits to insert on the posterior side of the humerus of the upper arm. As the latissimus dorsi approaches its insertion point, the many muscular fibers from its many origins merge to a point, giving the muscle a triangular shape.
The latissimus dorsi has several different functions, all of which involve movements of the arm. The primary function of the lat is the adduction of the arm, which is often used when performing a pull-up or chin-up or when pulling a heavy object down from a shelf above one’s head. Another function of the lat is extension of the arm, as in swinging the arm toward the back. This motion is used when swinging the arms while walking as well as during rowing exercises. Finally, the latissimus dorsi medially rotates the arm, moving the front of the arm towards the body’s midline. It also plays a role in extension and lateral flexibility of the lumbar spine and has an impact on pelvic positioning!
When this muscle becomes too tight, the opposite movements, from the ones listed above, can become inhibited. When this happens, the body's natural response is to compensate so the desired movement can be accomplished. Injury and misalignments like rounded shoulders or wrong positioning of lower back and pelvic occur when our body has to make these compensations.
Having trouble with your overhead lifts? Experiencing shoulder pain, back pain, even wrist pain when attempting these lifts? Tight lats could be part of the issue!
On the picture you can see different myofascial release techniques of the latissimus dorsi muscle.
SHOULDER PAIN SERIES 14/23 - THE SERRATUS ANTERIOR MUSCLE:
The serratus anterior muscle also known as the ´boxers muscle´ originates on the top surface of the eight or nine upper ribs and inserts exactly at the anterior surface and medial border of the scapula. The muscle has three sections: the superior, intermediate or medial, and the inferior. The function of the serratus anterior muscle is to allow the forward rotation of the arm and to pull the scapula forward in protraction and around the rib cage. The scapula is able to move laterally due to the serratus anterior muscle, which is vital for the elevation of the arm. The serratus anterior muscle also allows the upward rotation of the arm, which allows a person to lift items over their head. It is intimately connected to the Rhomboids and makes a sling for the Scapula to balance between protraction and retraction! Unfortunately it is a muscle that commonly gets overlooked!
When this muscle doesn't function properly, you can get winging of the shoulder blades, pain between or under the shoulder blades, pain with deep breathing, shoulder pain and difficulty reaching behind the back or overhead.
Winging of the shoulder blade is a physical finding where the inside border of the shoulder blade is lifting off the thorax. A healthy shoulder blade will lie flat against your rib cage and will not lift off through movement. Any deviation of the shoulder blade from normal will change the way in which the humerus articulates within its socket and as such predispose to injury! The major cause of this postural dysfunction is weakness or tightness in the serratus anterior muscle. This finding is typical in overhead athletes who are experiencing pain, but is also very commonly seen in patients who spend the majority of their day sitting, such as office workers, and those who spend the majority of their day in a hunched position such as dentists or dental hygienists!
In this case, training your rotator cuff muscles will not result in much benefit as you need to address the muscles responsible for holding your shoulder blade in a good position!
In my next posts I will show some specific exercises to hold the scapula in a good position - stay tuned!
On the picture you can see how I approach the serratus anterior muscle for a myofascial release treatment.
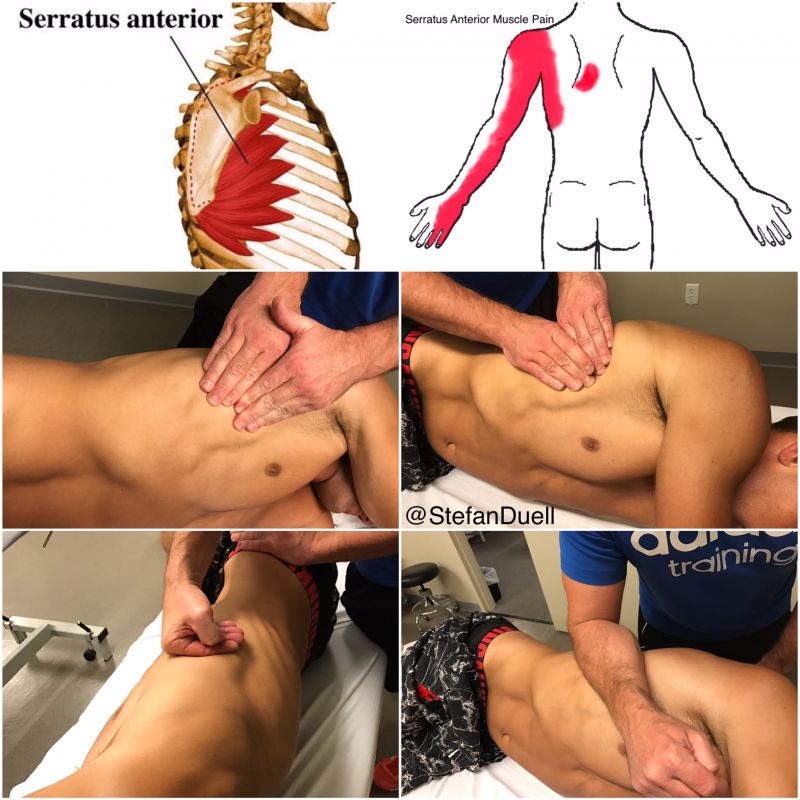
10. April 2017
Würzburg
SHOULDER PAIN SERIES 7/23 - PROTRACTED SHOULDER GIRDLE:
Protracted Shoulder Girdle and Automobilization with the Blackroll® and BLACKROLL® BALL:
Why your shoulders and thoracic spine are rounded?
Many people suffer nowadays from this alignment which is caused mainly by 2 key muscles: 1 the pectoralis minor and 2 the lower trapezius muscle (ascending part of the trapezius). 1 The pectoralis minor runs from the coracoid process down to ribs 3-5. It will become adaptively short when sitting at the desk, working with computers, favor exercises such as the bench press or other pressing exercises etc., which most people do! Being in poor positions and using the pecs will cause this adaptative shortening and tightness. When the pec minor is positioned short it will pull down on the scapula tilting it forward. It also will inhibit (weaken) the rhomboids, lower trapezius and serratus anterior which will lead to muscular imbalances!
2 The lower trap runs from vertebra T7-T12 up to the spine of the scapula. Normally this muscle pulls down on the scapula from the back creating a balancing act with the pectoralis minor for the scapula position. But if the pec minor is getting tight and short throughout poor positioning the lower trap gives up and gets weaker and weaker!
This poor alignment we are talking about can even lead to mechanical problems in the cervical spine or shoulder joint as it makes it very difficult to use the glenohumeral joint in centrated neutral position. That's why it is essential to work on it!
On the picture you can see different possibilities how to work by yourself on this problems with the @BLACKROLL® and @BLACKROLL® BALL releasing the pec minor and 2 variations of mobilizing your thoracic spine as well as 1 exercise to put some in the lower trap to activate it!

SHOULDER PAIN SERIES 8/23 - PROTRACTED SHOULDER GIRDLE - MYOFASCIAL RELEASE OF THE PECTORALIS MAJOR MUSCLE:
Regarding my yesterdays post about the 'Protracted Shoulder Girdle and Automobilization with the Blackroll® and BLACKROLL® BALL' I wanted to show some treatment techniques to my colleagues on how to work on that problem especially if the patient suffers from shoulder or cervical spine problems!
In the video you can see a myofascial release technique for the pectoralis major muscle. It is very important to perform the fascial technique from proximal to distal to lengthen the fascia of the pec major to give the shoulder girdle enough freedom to move back to the right position (Retraction + Depression)!
In my next posts I will talk about further specific treatment possibilities for therapists and self-treatment possibilities for patients if you suffer from shoulder pain - stay tuned!
SHOULDER PAIN SERIES 9/23 - PROTRACTED SHOULDER GIRDLE - MYOFASCIAL RELEASE OF THE PECTORALIS MINOR MUSCLE
.
Regarding my previous post about the Protracted Shoulder Girdle and Automobilization with the BLACKROLL® and Blackroll® BALL I wanted to show some treatment techniques to my colleagues on how to work on that problem:
.
Role of the pectoralis minor muscle?
The pectoralis minor runs from the coracoid process down to ribs 3-5. It will become adaptively short when sitting at the desk, working with computers, favor exercises such as the bench press or other pressing exercises etc., which most people do! Being in poor positions and using the pecs will cause this adaptative shortening and tightness. When the pec minor is positioned short or tight it will pull down on the scapula tilting it forward. It also will inhibit (weaken) the rhomboids, lower trapezius and serratus anterior which will lead to muscular imbalances. Further it can lead to thoracic spine, cervical spine or shoulder problems!
In the video you can see an active myofascial release technique for the pectoralis minor muscle by Dalton Myoskeletal Therapy. I experienced very good results with this technique, you should try it! Thanks to Erik Dalton for showing me that one!
SHOULDER PAIN SERIES 10/23 - PROTRACTED SHOULDER GIRDLE - MYOFASCIAL RELEASE OF THE PECTORALIS MINOR MUSCLE:
Check my yesterday's post about the myofascial release of the pectoralis minor muscle!
Here is another possibility regarding treatment: in this case the therapist is moving the arm of the client in abduction and adduction while the elbow of the opposite arm of the therapist is treating the pectoralis minor muscle.
SHOULDER PAIN SERIES 11/23 - PROTRACTED SHOULDER GIRDLE - MYOFASCIAL RELEASE OF THE PECTORALIS MINOR MUSCLE:
Another possibility regarding my previous post about the myofascial release of the pectoralis minor muscle:
Out of this position with your thumb you can perform 1 a trigger point technique, 2 a release technique between the fascia of pec major and minor or 3 a release technique for the complete pec minor muscle!
1 If you want to perform a trigger point technique make sure you hold the pressure as long the patient tells you the pain or the radiation goes down or the pain is not radiating anymore but at least for 1 minute and finish the technique then with a Ponçage. I usually hold the pressure until i feel a myofascial release under my finger!
2 If you decide to release the fascial connection between pec major and minor use your thumb or finger 2-4 and stay between pec major and minor until you feel a fascial release!
3 If you do the complete pec minor fascial release technique make sure you perform the technique from proximal to distal to lengthen the fascia of the pec minor to give the shoulder girdle enough freedom to move back to the right position (Retraction + Depression)!

07.-09. April 2017
Belgrade - Davis Cup - Serbia vs. Spain
Another great and successful week with an amazing team! Thank you Teniski savez Srbije for the invitation to work with this incredible athletes!
See you guys in September for Davis Cup by BNP Paribas semifinals vs. France!
#TeamSpirit #DavisCup #TeamSerbia #Physiotherapist








06. April 2017
Belgrade - Davis Cup - Serbia vs. Spain
Official Draw:


05. April 2017
Belgrade - Davis Cup - Serbia vs. Spain
Official Davis Cup by BNP Paribas dinner at world group quarterfinal Serbia vs. Spain in Belgrade at Novak's restaurant!
#DavisCup #TeamSerbia #Belgrade #TeamSpirit
SHOULDER PAIN SERIES 6/23 - MYOFASCIAL RELEASE OF THE SUPRASPINATUS MUSCLE
I m in Belgrade right now preparing with the Serbian Davis Cup by BNP Paribas team for the tie vs. Spain, thank you Dusan Lajovic Official for the pictures!
Regarding to my previous post about the Impingement Syndrome I wanted to focus on the supraspinatus muscle and show some treatment possibilities.
The supraspinatus muscle is one of the four rotator cuff muscles and the one most susceptible to injury. When someone tells me they are having a shoulder problem I ask, “Does it hurt to put your jacket on?” If the answer is yes, the overwhelming odds are that the injury is to the supraspinatus muscle and/or tendon.
The four muscles of the rotator cuff are the supraspinatus, supscapularis, teres minor and the infraspinatus. The tendons of these muscles act like ligaments in a way that no other muscle in the body does, and as a result makes them more vulnerable to injury.
The supraspinatus muscle follows the top of the shoulder blade attaching to the top of the humerus, the arm bone. The muscle helps to lift the arm up and is essential to all throwing actions, which is why it is the bane of so many athletes. When the supraspinatus muscle engages or shortens, the arm is pulled sideways away from the body. It also helps to stabilize the shoulder joint keeping the humerus pressed firmly into the shoulder blade.
On the pictures you can see how I approach the supraspinatus muscle for a myofascial trigger point treatment. In this case the 'Small Bevelled-Tip T-BAR' (St. John NMT) is very useful for releasing the tendon, the muscle stomach or even the subacromial space where the tendon or bursa can get entrapped!
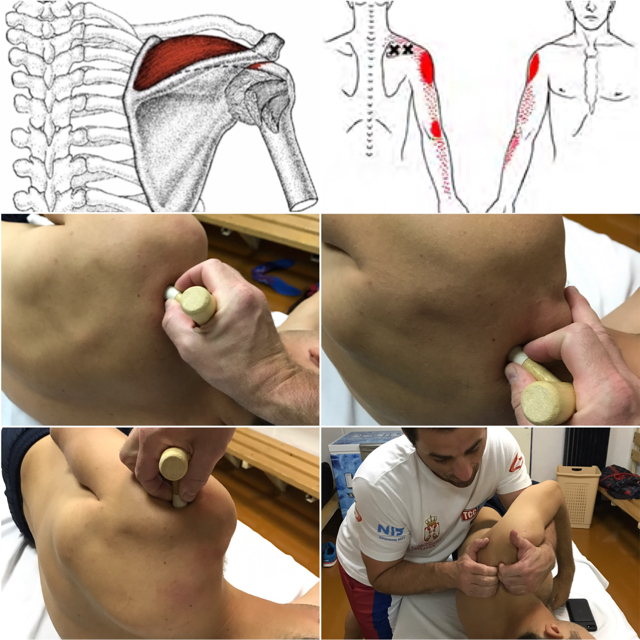
04. April 2017
Belgrade - Davis Cup - Serbia vs. Spain
Can't wait to absorb some incredible positive energy the upcoming week! Looking forward to join the serbian Davis Cup by BNP Paribas team in a few hours! On my way to Belgrade to support my friends at the quarterfinals tie Serbia vs. Spain. Proud to be a member of one of the best national tennis teams of the world!
#DavisCup #TeamSerbia #SRBvsESP #Physiotherapist

03. April 2017
Würzburg
Great post from my colleague @adam__rehab regarding anatomy trains / myofascial meridians which appear in the human body (described by Thomas Myers: Anatomy Trains). Check this post for better understanding of the way of thinking described in my last 2 posts on 'THORACIC ROTATION AUTOMOBILIZATION EXERCISE (SELF-TREATMENT)'.
ANATOMY TRAINS
These are also known as myofascial meridians and provide an explanation of how the body moves as a whole body myofascial tensegrity system instead of individual muscles and levers.
They were developed by Tom Myers of @anatomytrainsofficial in the 1990's when he was teaching at the Rolf Institute as a way of showing his students the myofascial connection of tissue through the body.
They are considered lines of pull which distribute strain, transmit force and effect the structure and function of the body.
They displayed as a series of Myofascial Lines:
SFL-Superfical Front Line
SBL-Superficial Back Line
LL-Lateral Line
SPL-Spiral Line
DFL-Deep Front Line
AL-Arm Lines x 4
BFL-Back Functional Line
FFL-Front Functional Line
These lines can be incorporated in movement practices such as Pilates or Yoga as well as Personal Training, Physiotherapy and Rehabilitation and any Stretching or Strengthening routines.
#AnatomyTrains #Physiotherapy #Osteopathy #Deutsches Fortbildungsinstitut für Osteopathie
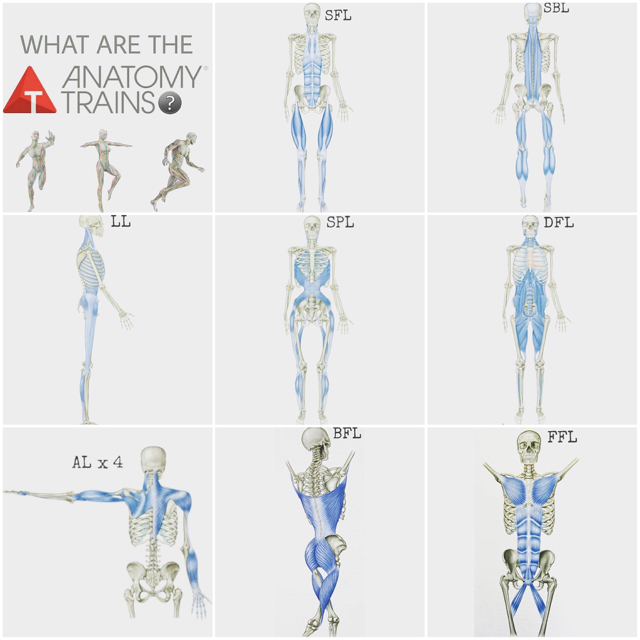
Just received this awesome delivery: BLACKROLL® foam rollers especially prepared for the Serbian Davis Cup by BNP Paribas team including flag. Thank you so much Blackroll® for the support! Ready to head out to Belgrade!
#Blackroll #DavisCup #TeamSerbia

SHOULDER PAIN SERIES 4/23 - LEVATOR SCAPULAE MUSCLE PAIN AND MYOFASCIAL RELEASE OF LEVATOR SCAPULAE MUSCLE:
The levator scapulae muscle resides at that back and side of the neck. Levator means to lift in Latin, so as the name implies, its goal is to lift the scapula. It comes up by tendinous slips from the transverse processes of the atlas and axis and from the posterior tubercles of the transverse processes of the third and fourth cervical vertebrae. It is embedded into the vertebral border of the scapula, amid the medial angle and the triangle smooth surface at the root of the spine.
Where do the levator scapulae muscle cause pain?
Levator scapulae muscle trigger points can lead to referred pain on the lateral side of the neck and in the shoulders as you can see on the red marked zones in the picture. You may feel burning between your shoulder blades after sitting at your computer without elbow support. .
What causes elevator scapulae muscle pain?
-Stress -> Relax those shoulders!
-Head forward posture -> Remember to sit up straight, lower your shoulders and bring your head back!
Holding a phone between your ear and shoulder -> Get a headset!
-Wrong training habits -> Shrugs!
-Bra straps that are too tight -> Have your bra fit by a person trained to get a good fit!
-Any position where your head is turned to one side ->Do you turn to see your computer screen?
On the picture you can see how I approach the levator scapulae muscle for a myofascial trigger point treatment.
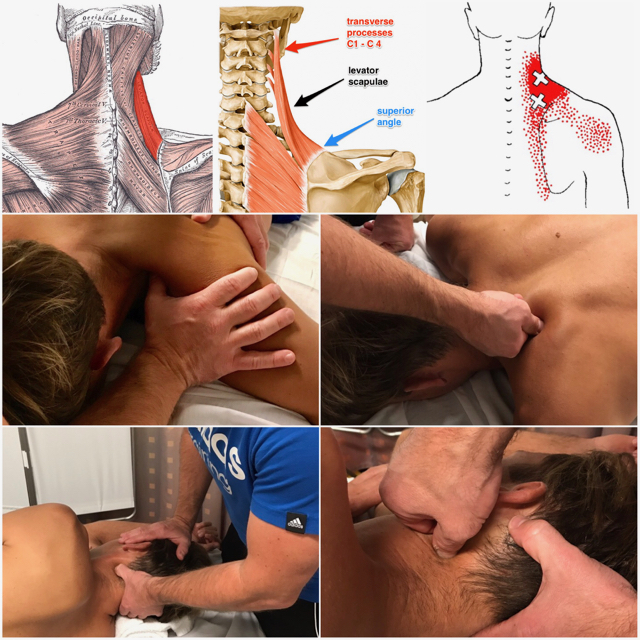
Great post by @dr.jacob.harden which actually fits exactly to my previous post on how to perform a self-treatment for the levator scapulae muscle!
.
#Repost @dr.jacob.harden
・・・
THIS MUSCLE IS A REAL PAIN IN THE NECK - SWIPE LEFT!
You know that knot at the base of your neck that everyone says is in their traps? It's not in your traps. It's deep to them in a muscle called the levator scapulae.
.
Levator connects from the upper inside border of the shoulder blade up into the neck. And when you spend hours looking down at your phone, computer, or desk, it gets brought onto stretch and placed under eccentric load.
.
Now since it has one stable attachment (the neck), and one mobile attachment (the scapula), which do you think is going to move? The shoulder blade of course. So when this muscle gets tensioned out, it will hike the shoulder up on that side. So here's a possible uneven shoulder fix too.
.
Use the release in this post for 30 seconds to 1 minute to help decrease some of the pain and tension through your neck and shoulder. Then tag a friend who needs this and share the wealth!

02. April 2017
Miami - Miami Open - ATP 1000
Thank you Miami, it was good as always but this time even better!!!
6 weeks USA ATP World Tour trip - on my way home for one day and Tuesday to Belgrade to support my serbian friends (Novak Djokovic, Janko Tipsarevic Official, Viktor Troicki, Nenad Zimonjić and Dusan Lajovic Official) at the Davis Cup by BNP Paribas quarterfinals tie Serbia vs. Spain! #TeamSpirit

01. April 2017
Miami - Miami Open - ATP 1000
Mission Miami Open accomplished!
Congrats to Marcelo Melo and Łukasz Kubot on an incredible run the last 4 weeks: runner-up at BNP Paribas Open and tournament win at Miami Open - Bravo! Keep it going guys! #TeamMeloKubot

31. March 2017
Miami - Miami Open - ATP 1000
Regarding my yesterdays post about 'Strengthening the Core Muscles`I wanted to show some more exercises which are very helpful if you suffer from back problems!
Mobility, Flexibility and Stability of the spinal system are very important aspects to watch at! The 'Lower Trunk Rotation' and 'Upper Trunk Rotation' exercises as shown on the picture can help to manage it!
Don't forget to activate your core muscles before you start doing this exercises but also in general before exercising like I explained in yesterday's post.
Good muscular control of the core and spine is the!
#Core #Stabilization #InjuryPrevention

SHOULDER PAIN SERIES 1/23 - TRAINING ADVICE:
If you suffer from shoulder pain, check your training habits!
#Repost @vinnierehab
'WHY SHRUGS COULD BE THE SOURCE OF YOUR SHOULDER PAIN!?
The legendary "shrug" exercise has been a gym staple in the strength and conditioning world forever!
Muscular development is a sure thing with this exercise but lets be on the same page with what primary muscles are contracting and what underlying dysfunction can come as a result
Although we may think that the UPPER TRAP depicted on the bottom left is the primary player, it is more dominantly the LEVATOR SCAPULAE depicted on the bottom right which majorly controls this action
People with anterior shoulder pain + mechanical dysfunction of the shoulder usually have downwardly rotated shoulder blades and you guessed it...The levator is an aggressive shoulder blade (scapula)downward rotator
If you didn't know before now you know that your shoulder blade is very likely the root of your shoulder pain and an exercise like this can be reinforcing an injury prone shoulder blade position!''
In my next posts I will talk about specific treatment possibilities for therapists and self-treatment possibilities for patients if you suffer from shoulder pain - stay tuned!
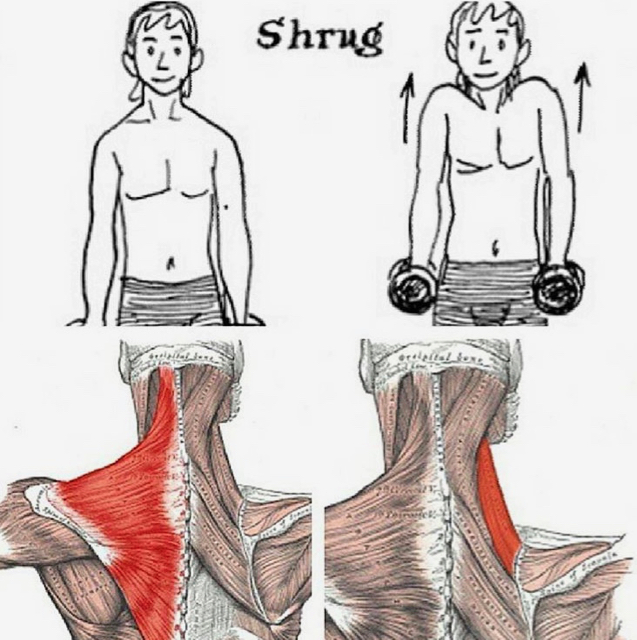
SHOULDER PAIN SERIES 2/23 - TRAPEZIUS MUSCLE PAIN AND MYOFASCIAL RELEASE:
Your trapezius muscles are some of the first to bother you when you are under stress. They ache and burn from the base of your skull to between your shoulder blades. The good news is that the pain is relatively easy to get under control!
When we are under stress, one of the first muscles to cause us pain is our trap muscles, and part of that reason is because of the role they play in our movement.
The trapezius is a broad triangular muscle which attaches to the base of the skull, and lies at the back of the neck, over the upper shoulders and extends down your upper back to your mid back. It is one of the most likely muscles to get sore knots or “trigger points”.
The trap muscles are the only muscles which can lift the outside of your shoulders to create a “shrug”. They move the head and neck toward the shoulder of the other side. The middle of the muscles pull the shoulder blades together, while the lower draw the shoulder blades downward. They support the weight of the arms.
Often these movements are at play when we are under stress, and doing the activities that cause stress.
Where do the trapezius muscle cause pain?
Trap pain is classic stress pain. Your shoulders ache and your neck hurts. You may have a headache, especially in the temples or behind your eyes or at the base of your skull. You may feel burning between your shoulder blades after sitting at your computer without elbow support. The trapezius muscle trigger points can lead to referred pain in the shoulders and head as you can see on the red marked zones in the picture.
What causes trapezius muscle pain?
- Stress -> Relax those shoulders!
- Head forward posture -> Remember to sit up straight, lower your shoulders and bring your head back!
- Holding a phone between your ear and shoulder -> Get a headset!
- Wrong training habits -> Shrugs!
- Bra straps that are too tight -> Have your bra fit by a person trained to get a good fit!
- Any position where your head is turned to one side -> Do you turn to see your computer screen!
SHOULDER PAIN SERIES 3/23 - MYOFASCIAL RELEASE OF THE TRAPEZIUS MUSCLE AND OSTEOPATHIC VIEW:
The trapezius muscle is one of the largest superficial muscles that extend longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to the spine of the scapula. Its functions are to move the scapulae and support the arm. The trapezius has three functional regions: the superior region (descending part), which supports the weight of the arm; the intermediate region (transverse part), which retracts the scapulae; and the inferior region (ascending part), which medially rotates and depresses the scapulae. Contraction of the trapezius can have two effects: movement of the scapulae when the spinal origins are stable, and movement of the spine when the scapulae are stable. Its main function is to stabilize and move the scapula.
This muscle tends to develop too much tension for postural reasons, such as forward head posture (where it has to work overtime to stabilise the head and neck due to poor alignment). Other reasons include poor breathing patterns (shallow neck breathing all day), and muscle imbalances elsewhere.
The trapezius muscle trigger points can lead to referred pain in the shoulder region and head (headache) as you can see on the red marked zones in the picture. They also can initiate trigger points in the jaw joint muscles. Additionally, the muscle can cause biomechanical problems in the cervical and thoracic spine.
The trapezius is innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen, where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the trapezius. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly.
On the picture you can see several myofascial treatment techniques for the trapezius muscle incl. the jugular foramen release.
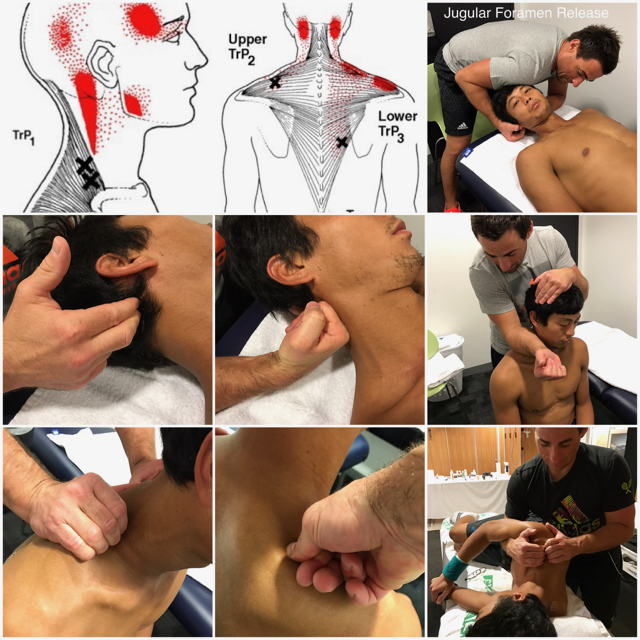
30. March 2017
Miami - Miami Open - ATP 1000
Strengthening the Core Muscles:
Very important for every athlete to prevent injuries as well as for everyone who is suffering from lower back or lower extremity problems!
People with low back pain, past and present, have been shown to have poor motor control and activation of their transversus abdominis (TrA) and multifidus (MF) muscles.
First, what do these muscles do? They work with the diaphragm and pelvic floor to adjust the intraabdominal pressure - affecting the spine stability - and control intersegmental motion of the spine. Meaning they help keep your spine in the right place!
TrA and MF are active during all functional tasks. The central nervous system (CNS) sends messages to activate these muscles before predictable movements, and to react to unexpected movements. So the right timing in use of these muscles is important!
Working on your TrA and MF activation is an important step in improving and preventing that annoying recurring low back pain.
Good muscular control of the core and spine can help reduce instability and pain!
These exercises, which are best learned with a physical therapist, consist of the following:
1-Finding the position the spine is most comfortable in (neutral spine)
2-Educating the back muscles to keep the spine in the neutral position (MF muscles)
3-Educating how to contract the TrA muscle
4-Educating how to contract the pelvic floor
5-Educating how to contract the thoracic diaphragm
6-Maintaining the neutral position through a series of movements that apply more and more degrees of freedom of motion.
Dynamic lumbar stabilization exercises are commonly prescribed for any kind of lumbar problems and even for reducing sciatica-type pain from degenerative disc disease, or pain that radiates into the buttock and/or down the back of the leg.
#Stability #Training #LumbarStability #Core #Stabilization#InjuryPrevention #Physiotherapy #Osteopathy
29. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 14/15: THORACIC ROTATION AUTOMOBILIZATION EXERCISE (SELF-TREATMENT)
Your thoracic spine needs to be mobile - our body is smart and will find to get that motion from somewhere else! Those areas of compensation might lead to poor movement patterns, overuse and pain.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include thoracic mobilization exercises in your daily training routine!
This post describes how to mobilize the thoracic spine included in the mobilization of 'The Posterior Spiral Line' by @AnatomyTrainsOfficial:
You don't even need a training device as you can perform it with a simple automobilization exercise! Flexibility is very important and it keeps the fascial connective tissue in good condition as well as to prevent injuries! Stretching is a 'Must Do' for every athlete and human being!
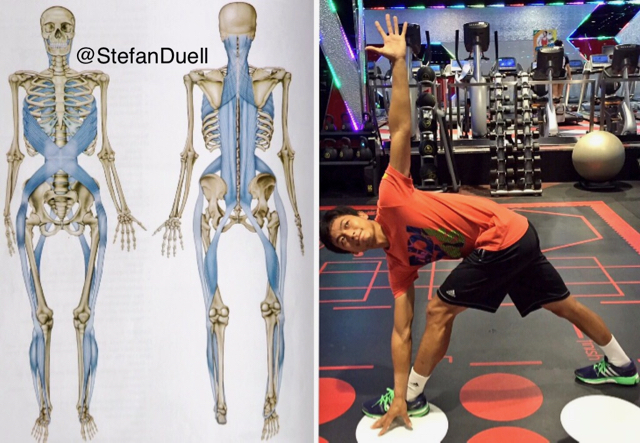
THORACIC SPINE (T-SPINE) SERIES 15/15: THORACIC ROTATION AUTOMOBILIZATION EXERCISE (SELF-TREATMENT)
Your thoracic spine needs to be mobile - our body is smart and will find to get that motion from somewhere else! Those areas of compensation might lead to poor movement patterns, overuse and pain.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include thoracic mobilization exercises in your daily training routine!
This post describes how to mobilize the thoracic spine included in the mobilization of 'The Anterior Spiral Line' by @AnatomyTrainsOfficial:
Use the @TRXtraining T-Spine Rotation Exercise which is a simple active thoracic spine automobilization everybody can perform! It is very important to keep the fascial connective tissue in good condition as well as to prevent injuries!
28. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 12/15: SEGMENTAL THORACIC EXTENSION AUTOMOBILIZATION EXERCISE WITH THE BLACKROLL® (SELF-TREATMENT)
In my previous posts about the thoracic spine I showed mainly the treatment techniques for my colleagues on how to work on misalignments in this part of the human body. Following on, I will provide some input to you all out there on how to work on it by your own especially after receiving some treatment to keep up the balance ⚖ - stay tuned!
The thoracic spine is built from its anatomical structure to be mobile! That's why it is very important to keep it mobile and even to visualise and feel the possible movement in the thoracic spine. Many people don't even know or just are not able to feel that there is a specific movement possible, for visualising this movement the Blackroll® is an excellent training device.
Your spine needs to be mobile - our body is smart and will find to get that motion from somewhere else! Those areas of compensation might lead to poor movement patterns, overuse and pain.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include this mobilization exercise, together with a pectoralis muscle stretching exercise, in your daily training routine. Because if the pectoralis muscle is locked short it won't be possible to mobilize the thoracic spine properly!
1-Roll out your back for 1 minute
2-Start with your roller at the beginning of your lumbar spine
3-Bend your arms in the elbow and extend over the roller
4-Work segmentally up to your cervical spine and then back
5-It's ok to pause into the extension and allow your spine to relax over the roller
THORACIC SPINE (T-SPINE) SERIES 13/15: SEGMENTAL THORACIC AUTOMOBILIZATION EXERCISE FOR ROTATION (SELF-TREATMENT)
Your thoracic spine needs to be mobile - our body is smart and will find to get that motion from somewhere else! Those areas of compensation might lead to poor movement patterns, overuse and pain.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include this mobilization exercise in your daily training routine.
Make sure you mobilize your thoracic spine! This exercise helps increase rotation through your mid back. In the video you see a T-Spine rotation exercise from a 4 point position:
1-Sit back towards your heels to create a lumbar lock ensuring that the movement occurs through your thoracic spine and start in a rotated position towards your stabilizing arm.
2-Rotate away from your supporting arm drawing your shoulders round at the same time as retracting your shoulder blade.
3-Do it 15-20 times each side, if you find one side more restricted then the other add 5-10 more reps.
Simple and effective exercise everybody can perform!
27. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 9/15: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE THORACO-LUMBAR-JUNCTION HVLA
The T12-L1 spinal segment, also referred to as the thoraco-lumbar-junction (TL Junction), is located at the very bottom of the thoracic spine.
More specifically, this is where the thoracic spine connects with the lumbar spine.
A TL Junction subluxation requires a distraction mobilization. First of all you should make sure to have released all myofascial structures which cause a TL Junction subluxation as I explained in my previous post about the intrinsic back muscles. Usually if you do a proper myofascial release treatment the TL Junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems.
The patient stands and places his hands behind the neck and then the therapist wheels through the space in front of the shoulders and applies a distraction force via the therapists sternum through the TL Junction.
THORACIC SPINE (T-SPINE) SERIES 10/15: THE IMPORTANCE OF THE FIRST RIB + MYOFASCIAL AND MANUAL THERAPEUTIC TREATMENT
The first rib has a very distinct shape. Due to the shape of the articular facet on the transverse process of the first thoracic vertebrae being oriented slightly upwards, the weight of the first rib is supported below leading to most deviations of the first rib to be upwards. There is a groove for the subclavian artery and the subclavian vein. As the subclavian artery and vein pass laterally to the first rib they become the axillary artery and vein. Also present are the superior intercostal artery and vein.
The muscles that attach to the first rib are: subclavius, anterior/middle scalene, serratus anterior and levator costae. The job of these muscles is either to fix the rib in place or draw it upwards.
Nerves that are related to the first rib are: the median nerve, the radial nerve, the lateral pectoral nerve, the thoracodosal nerve, the ulnar nerve, the stellate ganglion, the first intercostal nerve, and the recurrent meningeal nerves. Also, due to the relationship with the head of the first rib, the inferior cervical ganglion is affected by the first rib.
Due to the relationship with the clavicle, the first rib has a great affect on the lymphatic drainage of the entire body via the thoracic duct and the right lymphatic duct.
Symptoms of a subluxated/blocked first rib:
- Muscular contracture related to the nerves at C8 and T1 as well as causing muscular contracture of neck muscles.
- Pain in the arm and along the first intercostal space.
- Functional disturbances of the heart (via nervous connections including the vagus nerve as it passes between the subclavian artery and vein).
- Lung and bronchial disturbances (more common than heart disturbances) due to the nervous connections.
- Disturbed vasomotion to the head and face via disturbances to the gangliated cord.
- Throat issues due to the inferior cervical ganglion and its connection with the laryngeal nerves (often creating a hacking cough).
- The thyroid gland is often disturbed through the connections of the stellate and inferior cervical ganglia by way of altering the vasomotion leading primarily to congestion and hypertrophy (the rib impinges and causes facilitation to the nerves leading to increased blood flow).
Considering the above noted conditions it is clear that proper articulation of the first rib is very important. Due to the nature of the articulation, attempting to “lower” the first rib may not be appropriate. Instead it is more likely that removal of the contracture of the muscles on the superior surface (neck muscles) is a more appropriate methodology for relieving a dis-articulated first rib. It is also vitally important that the clavicle be lifted from the first rib to ensure that the structures beneath it are not obstructed. Consider that the head, face, neck, heart, and lungs can all be directly affected by the first rib.
On the picture you can see several myofascial release techniques for the scalene muscles and the subclavius muscle which can cause biomechanical problems in the thoracic and cervical spine, due to its influence on the first rib in terms of elevating it, as the rotation in the thoracic and cervical spine will be irritated. You can see as well a manual mobilization technique of the first rib.
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)

THORACIC SPINE (T-SPINE) SERIES 11/15: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE FIRST RIB HVLA
A blocked or subluxated first rib requires a mobilization.First of all you should make sure to have released all myofascial structures which cause a elevated first rib as I explained in my previous post about 'THE IMPORTANCE OF THE FIRST RIB + MYOFASCIAL AND MANUAL THERAPEUTIC TREATMENT'. Usually if you do a proper myofascial release treatment the first rib will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems.
The video shows how I manipulate a blocked first rib, we will assume a restriction of the right first rib. With the patient in prone position the therapist stands at the top of the patients head. The therapist moves the head of the patient in cervical spine extension and turns the head with his left hand to the left side (cervical spine rotation to the right). With his right thenar placed on the rightt first rib, the therapist now performs a high velocity low amplitude (HVLA) thrust towards the table.
26. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 7/15: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE UPPER THORACIC SPINE SUPINE HVLA
An upper thoracic spine subluxation requires a mobilization. First of all you should make sure to have released all myofascial structures which cause an upper thoracic spine subluxation as I explained in my previous post about the intrinsic back muscles. Usually if you do a proper myofascial release treatment the upper thoracic spine subluxation will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems.
We will assume a restriction at T2/3 on the left:
With the patient supine the therapist stands to the right of the patient. The patient crosses the hands behind the neck to creating stability allowing the therapist to introduce flexion to the level of dysfunction. The therapist makes a fulcrum fist with the right hand which is then placed underneath the patient with the spinous processes of T2 to T3 within. Compression is added via the therapists sternum. Through the patients flexed elbows a thrust is then delivered once the forces are focused down the line of the patients arm via the glenohumeral joint through the fulcrum hand. The force can be focused further by adding the principles of minimal leverage and enhanced by using breathing.
THORACIC SPINE (T-SPINE) SERIES 8/15: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE LOWER THORACIC SPINE SUPINE HVLA
A lower thoracic spine subluxation requires a mobilization. First of all you should make sure to have released all myofascial structures which cause an upper thoracic spine subluxation as I explained in my previous post about the intrinsic back muscles. Usually if you do a proper myofascial release treatment the c-t-junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems.
We will assume a restriction at T9,10 on the left:
With the patient supine the therapist stands to the right of the patient. The patient crosses the elbows in front of the chest creating stability allowing the therapist to introduce flexion to the level of dysfunction. The therapist makes a fulcrum fist with the right hand which is then placed underneath the patient with the spinous processes of T9 to T10 within. Compression is added via the therapists sternum. Through the patients crossed elbows a thrust is then delivered once the forces are focused through the fulcrum hand. The force can be focused further by adding the principles of minimal leverage and enhanced by using breathing.
25. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 4/15: THE IMPORTANCE OF THE INTRINSIC BACK MUSCLES (AUTOCHTHONOUS BACK MUSCLES) + MYOFASCIAL TREATMENT
The muscles of the back can be divided into three groups – superficial, intermediate and intrinsic:
Superficial – associated with movements of the shoulder.
Intermediate – associated with movements of the thoracic cage.
Deep – associated with movements of the vertebral column. The deep muscles develop embryologically in the back, and are thus described as intrinsic muscles. The deep muscles of the back are well-developed, and collectively extend from the sacrum to the base of the skull. They are associated with the movements of the vertebral column, and the control of posture. The muscles themselves are covered by deep fascia, which plays a key role in their organisation.
Anatomically, the deep back muscles can be divided into three layers: superficial, intermediate and deep.
The superficial muscles are also known as the spinotransversales. There are two muscles in this group – splenius capitis and splenius cervicis. They are both associated with movements of the head and neck.
There are three intermediate intrinsic back muscles – the iliocostalis, longissimus and spinalis. Together these muscles form a column, known as the erector spinae. The erector spinae is situated posterolaterally to spinal column, between the vertebral spinous processes and the costal angle of the ribs.
All three muscles can be subdivided by their superior attachments, into: lumborum, thoracic, cervicis and capitis.
The deep intrinsic muscles are located underneath the erector spinae. They are a group of short muscles, associated with the transverse and spinous processes of the vertebral column. There are three major muscles in this group: the semispinalis, multifidus and rotatores.
This deep muscles can cause subluxations in the facet joints of the thoracic spine, that's why it is very important to apply a proper myofascial release treatment on these structures. Usually I do not use a lot of treatment devices, but in this case the Small Bevelled-Tip T-BAR (St. John Neuromuscular Therapy) is very useful!
On the picture you can see several myofascial release techniques for the thoracic intrinsic muscles.

THORACIC SPINE (T-SPINE) SERIES 5/15: MANUAL THORACIC SPINE EXTENSION MOBILIZATION
The thoracic spine is built from its anatomical structure to be mobile for rotation, flexion and extension! That's why it is very important to keep it mobile and even to visualise and feel the possible movement in the thoracic spine. Many people don't even know or just are not able to feel that there is a specific movement possible. But it has to be known because the thoracic spine must be used and must be moved! If people are unable to visualise and feel the movement of the thoracic spine, they will find another way to get that motion from somewhere else like lumbar spine, cervical spine or shoulder blades because our body is smart and very good in compensating. Those areas of compensation might lead to poor movement patterns, overuse and pain!
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include mobilization exercises and stretching exercise in your daily training routine!
Regarding my yesterdays post about `THE IMPORTANCE OF THE INTRINSIC BACK MUSCLES` I wanted to show a very effective mobilization technique on how my colleagues can work on a better extension in the T-Spine of their patients. If your patient suffers from this misalignment it is necessary to do a proper myofascial release treatment followed by a manual thoracic spine extension mobilization as you can see in this video!
THORACIC SPINE (T-SPINE) SERIES 6/15: OSTEOPATHIC DISTRACTION MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE CERVICO-THORACIC-JUNCTION HVLA
The C7-T1 spinal segment, also referred to as the cervico-thoracic-junction (CT Junction), is located at the very bottom of the neck.
More specifically, this is where the neck (cervical spine) connects with the upper back (thoracic spine).
A CT Junction subluxation requires a distraction mobilization. First of all you should make sure to have released all myofascial structures which cause a CT Junction subluxation as I explained in my previous post about the intrinsic back muscles. Usually if you do a proper myofascial release treatment the CT Junction will correct itself but sometimes it can still stay subluxated. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the joint to the right position otherwise it can force thoracic, cervical or shoulder problems.
The patient is seated, almost the same hight then the therapist. The patient places his hands behind the neck and then the therapist wheels through the space in front of the shoulders and applies a distraction force!
24. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 3/15: NERVOUS SYSTEM AND VISCERAL INFLUENCE OF A THORACIC FACET JOINT SUBLUXATION
Facet joints are small joints at each segment of the spine that provide stability and help guide motion. The facet joints can become painful due to arthritis, a back injury, mechanical stress to the back or misalignment (subluxation). The facet joints are paired joints in the back and neck, one pair at each vertebral level (one joint on each side of the vertebrae). These joints have opposing surfaces of cartilage and a surrounding capsule that is filled with synovial fluid, which reduces the friction between bones that rub together.
A thoracic facet subluxation can have a huge influence to the sympathetic nervous system which is located in the thoracic spine. It is one of the two main divisions of the autonomic nervous system, the other being the parasympathetic nervous system. The autonomic nervous system functions to regulate the body's unconscious actions.
The sympathetic nervous system's primary process is to stimulate the body's fight-or-flight response. It is, however, constantly active at a basic level to maintain homeostasis. It is controlling organs like the heart, lungs, stomach, liver, kidneys and intestines. If there is a subluxation your sympathetic nervous system isn't able to function optimally! Considering your nervous system is the master system of the human body and controls every cell, tissue and organ it is essential to correct that kind of misalignment very quickly!
Most conservative treatments for facet subluxation involves postural correction, soft tissue treatment and osteopathic manipulation of the affected areas. Physical therapists, osteopathic clinicians and chiropractors are adept at restoring restricted and painful facet joints to move and can reestablish normal motion.
In my next posts I will talk about specific myofascial and chiropractic treatment of thoracic facet joint problems - stay tuned!
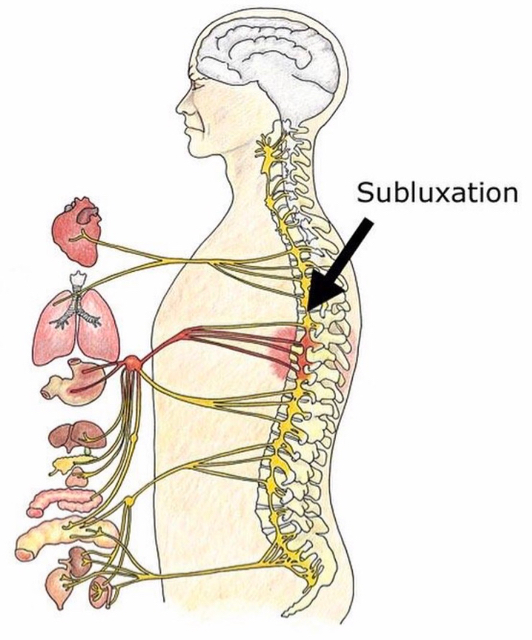
23. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 2/15: THE IMPORTANCE OF THE THORACIC DIAPHRAGM AND MYOFASCIAL TREATMENT
Diagnosis and treatment of the thoracic diaphragm muscle is very important not only if you work with professional athletes - it is very important for every human being!
The thoracic diaphragm muscle is the most important muscle of inhalation. The diaphragm separates the thoracic cavity, containing the heart and lungs, from the abdominal cavity and performs an important function in respiration: as the diaphragm contracts, the volume of the thoracic cavity increases and air is drawn into the lungs. It has a lot of very important fascial connections to the sternum, the ribs, the thoracic/lumbar spine, to abdominal organs as well as to an other very important muscle in our body - the iliopsoas muscle, which can cause a lot of problems too! There are three large openings in the diaphragm through which structures pass between the thorax and abdomen: the aortic, the esophageal and the caval opening plus a series of smaller ones which are very important for blood circulation and lymph circulation. The diaphragm is also involved in non-respiratory functions, helping to expel vomit, feces and urine from the body by increasing intra-abdominal pressure and even preventing acid reflux by exerting pressure on the esophagus as it passes through the esophageal hiatus. If you are familiar with the anatomy of the diahragm you will easily understand that it can cause spine or stomach problems, it can prevent injuries, increase endurance and even support recovery as this muscle is involved in breathing mechanism and blood circulation! The diaphragm muscle plays a very important role during the examination of the human body, especially when I am working with professional tennis players. If it has any restrictions, it can limit the movement especially in the THORACIC SPINE rotation and decrease the performance, and even increase the risk of injuries due to the fact that other parts of the human body have to compensate it!
#Physiotherapy #Osteopathy
(Treatment technique: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
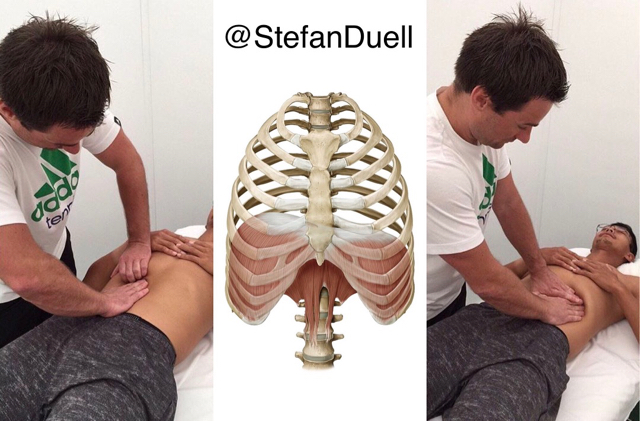
On my way to work!

22. March 2017
Miami - Miami Open - ATP 1000
THORACIC SPINE (T-SPINE) SERIES 1/15: THE IMPORTANCE OF THORACIC SPINE MOBILITY
The thoracic spine is built from its anatomical structure to be mobile for rotation, flexion and extension! That's why it is very important to keep it mobile and even to visualise and feel the possible movement in the thoracic spine. Many people don't even know or just are not able to feel that there is a specific movement possible. But it has to be known because the thoracic spine must be used and must be moved! If people are unable to visualise and feel the movement of the thoracic spine, they will find another way to get that motion from somewhere else like lumbar spine, cervical spine or shoulder blades because our body is smart and very good in compensating. Those areas of compensation might lead to poor movement patterns, overuse and pain!
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include mobilization exercises and stretching exercise in your daily training routine!
In my next posts I will talk about specific treatment possibilities for therapists and self-treatment possibilities for patients - stay tuned!
#Thoracic #Spine #Physiotherapy #Osteopathy
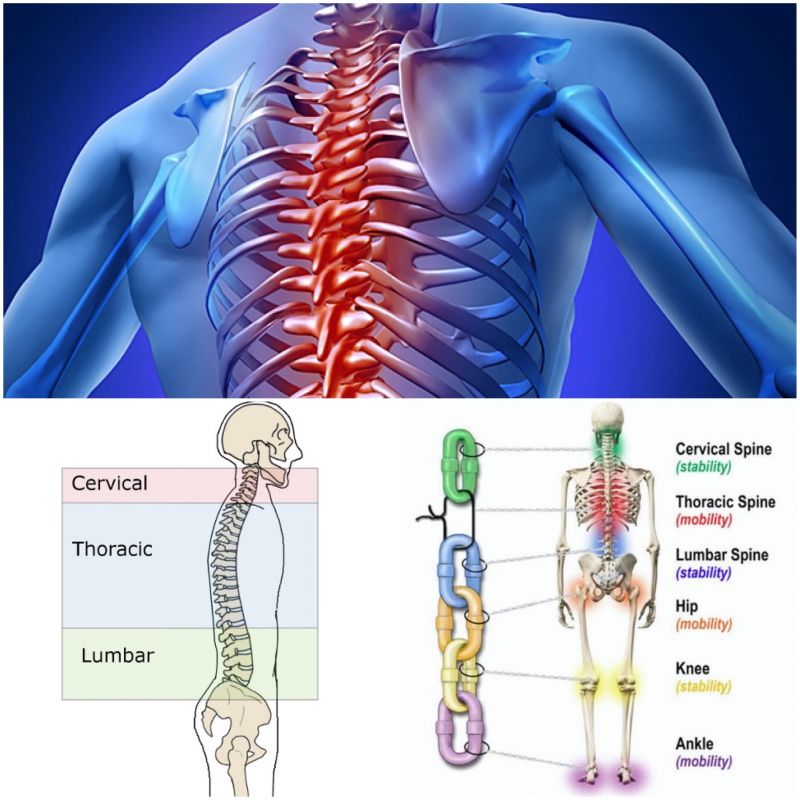
21. March 2017
Miami - Miami Open - ATP 1000
Thank you @vinnierehab for this post! I don't know how many discussions I had already with fitness coaches or even doctors about exactly this issue and unfortunately many of them just don't or don't want understand!
.
@vinnierehab
・・・
THE CRUNCH : Analysis + Advice
[A+A / CORE]
.
Who hasn't at some point in their life done thousands upon thousands of sit-ups / crunches in hope of having a sculpted midsection?
.
I remember when I was younger at karate school, the warm-up at the start of every class was 100 sit-ups and planks till you puked lol.
Ain't going to lie, as much as I don't think it was functional to do that back then, it definitely was a character builder, to push past the pain and keep going #feeltheburn
.
However, as you grow older, have injuries and more experience in this life, you realize that pushing through bad form and poor exercise programming is a silly idea!
.
Especially if you suffer from back pain, this exercise does nothing but compress your lumbar spine
.
This exercise according to some studies can cause hundreds of pounds of compression on the discs of your spine, and the repeated bending can potentially herniate your discs
.
To fully understand why this is a bad exercise, let's have a look at the function of the abs!
.
Common misconception out there is that people think the function of the abs is to flex the lumbar spine when really the abs mainly contract eccentrically in functional movement to DECELERATE extension of the spine in the sagittal plane
.
There is never a point in time in functional movement that your abs are asked to contract CONSCIOUSLY. Your core is meant to react to movement SUBCONSCIOUSLY as you go through life
.
That is why the crunch doesn't make sense as an exercise functionally because not only does it crush your spine, your body is never asked to do such a movement consciously
.
So if your goals are more functional than aesthetic, there is much better options out there that will not only get you looking shredded, but will also make you move like a ninja!!!
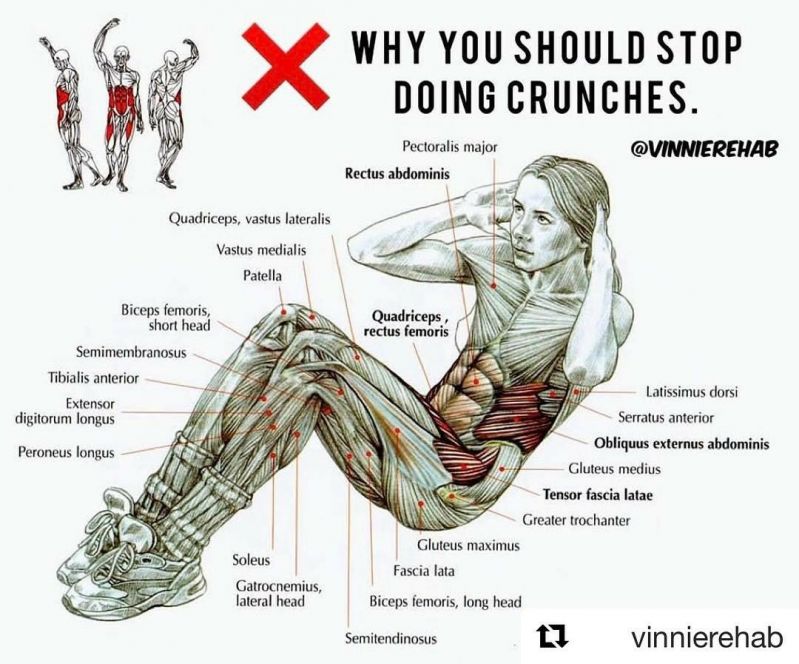
20. March 2017
Miami - Miami Open - ATP 1000
THE SACROILIAC JOINT SERIES 4/4: FOAM ROLLING WITH THE Blackroll® ON IMPORTANT STRUCTURES WHICH CAN FORCE LOWER BACK, HIP, KNEE AND FOOT PROBLEMS:
Some general information about foam rolling on the important muscles which keep the ilium bone in the anterior rotated position regarding my previous post: 'Osteopathic Manipulation of the Sacroiliac Joint using the Chicago Technique HVLA'.
How to perform a self myofascial release (self massage) to your muscles? Every foam rolling fanatic knows how to do it but it is very important to make sure to spend time on each of the individual muscles which keep the ilium bone in anterior rotated position (Iliacus muscle, Erector spinae muscles, Latissimus dorsi muscle, Adductor muscles, Rectus femoris muscle, Quadratus lumborum muscle, Tensor fascia latae muscle, gluteus medius muscle and External obturator muscle).
Make sure that you roll slowly among each muscle, trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Continue this process on each muscle until it feels as though you have an improvement or a decrease in general tightness. Ensuring you roll each muscle from the origin to the insertion is a good way to target the entire length of the muscle.

19. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
THE SACROILIAC JOINT SERIES 3/4: OSTEOPATHIC MANIPULATION OF THE SACROILIAC JOINT USING THE CHICAGO TECHNIQUE HVLA
An anterior rotated Ilium bone causing a functional long leg requires posteriorization. First of all you should make sure to have released all myofascial structures which cause an anterior rotation of the ilium bone: Iliacus muscle, Erector spinae muscles, Latissimus dorsi muscle, Adductor muscles, Rectus femoris muscle, Quadratus lumborum muscle, Tensor fascia latae muscle, gluteus medius muscle and External obturator muscle. Usually if you do a proper myofascial release treatment the ilium will correct itself but sometimes it can still stay anteriorized. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the ilium bone to the right position otherwise it can force lower back problems through an so-called ascending kinematic chain or even knee or foot problems through a descending kinematic chain.
The therapist stands on the opposite site of the dysfunction, you move the shoulders of the patient so that the upper torso is sideband away. Have the patient interlace the fingers behind the back of the neck. You now cross the leg of the opposite site over the leg nearest to you and then move the legs towards the opposite site of the table hints the patient is smiling away. This helps to focus the force at the left/right sacroiliac joint. You now insert your hand between the flexed arm of the patient that your dorsum is resting on the sternum. Introduce rotation through your arm pivoting the shoulder and the patients upper torso towards you. Place the caudal hand over the anterior superior iliac spine on the opposite site, continue rotation from above until the force is felt to accumulate under your caudal hand. Perform a high velocity low amplitude (HVLA) thrust with the caudal hand. The vector force is towards the opposite site of the table. Do not overrotate as the force will not accumulate at the sacroiliac joint!
18. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
THE SACROILIAC JOINT SERIES 2/4: OSTEOPATHIC MANIPULATION OF THE SACROILIAC JOINT USING THE LUMBAR ROLL TECHNIQUE HVLA
A posterior rotated Ilium bone causing a functional short leg requires anteriorization. First of all you should make sure to have released all myofascial structures which cause an posterior rotation of the ilium bone: Hamstring muscles, Gluteus maximus muscle, Rectus abdominis muscle, Obliquus externus abdominis muscle and Adductor magnus muscle. Usually if you do a proper myofascial release treatment the ilium will correct itself but sometimes it can still stay posteriorized. If so, it requires a high velocity low amplitude (HVLA) thrust technique to get the ilium bone to the right position otherwise it can force lower back problems through an so-called ascending kinematic chain or even knee or foot problems through a descending kinematic chain.
For the examination of the sacro iliac junction is it important to know your anatomical landmarks! You wind down the upper body of the patient below the lumbo sacral junction plus adding flexion and rotation. This focuses the force at the superior pole of the sacro iliac joint. Using the forearm you come over the superior pole of the posterior superior iliac spine (PSIS). Now you perform a high velocity low amplitude thrust towards the therapist thereby gapping the sacro iliac joint to a neutral position.
17. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
THE SACROILIAC JOINT SERIES 1/4: SACROILIAC JOINT DYSFUNCTION AND PAIN
Low back pain is very common, the sacroiliac joint (SI-Joint) is a major source of lower back pain. Pain originating from the SI-Joint is usually unappreciated, underdiagnosed, misunderstood and usually intributed to other sources such as the hip and spine! Patients experiencing lower back pain can spent months or even years in treatment without the correct diagnosis. Diagnostic injection at the SI-Joint is the only means to confirm diagnosis. Pain from the hips, spine and SI-Joint can overlap in the associated regions. If the patient has a back problem and it doesn’t improve for several months it is important to look at the SI-Joint!
The SI-Joints are weight bearing joints, these joints distribute weight from the spine to the lower extremities through the hip joints. From the front the SI-Joint is supported by the sacroiliac ligaments. There are also strong muscles (Psoas, Iliacus) and important nerves (Lumbosacral plexus) for the thigh and leg in front of the SI-Joint.
From the back the SI-Joint has strong posterior ligaments, the sciatic nerve crosses underneath the piriformis muscle, all this is covered by strong back muscles (Iliocostalis muscle, Longissimus thoracic muscle)
Symptoms:
-lower back, buttock, back of thigh and knee pain
-occasional groin pain
-difficulty and discomfort while sitting
-patient frequently changes position to become comfortable
Differential Diagnosis:
-Piriformis Syndrome
-Myofascial Pain
-Lumbosacral Disc Herniation
-Lumbosacral Facet Syndrome
Causes:
-Leg length discrepancy
-Mechanical dysfunction (Misalignment)
-Arthropathy
-Stomach or Gastro-intestinal adhesions (Osteopathic view)
Treatment:
-Anti-inflammatory medication
-Physical therapy, Osteopathy, Chiropractic, Medical training therapy
-SI-Joint injections: PRP (platelet rich plasma)
SI-Joint misalignment can force lower back problems through an so-called ascending kinematic chain ⛓or even knee or foot problems through a descending kinematic chain⛓ as you can see in the picture!
I usually treat the SI-Joint by using visceral, myofascial and chiropractic techniques after doing a proper osteopathic diagnosis as I will explain in further posts!
#SacroIliacalJoint #SIJoint #Physiotherapy #Osteopathy
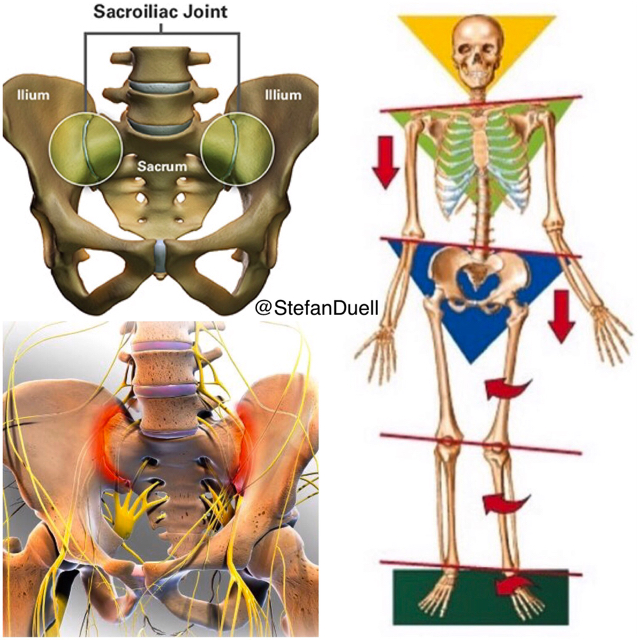
16. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
Thank you for 100 thousand views on my previous Instagram post! @StefanDuell
I wanted to share another great taping technique to support the foot and the calf in terms of injury prevention or even if you suffer from an injury like plantar fasciitis, achilles tendinitis or a calf muscle strain/tear.
Dynamic Tape to support the longitudinal arch of the foot incl. the achilles tendon and the calf muscle.
In that case the tennis player suffered from a calf muscle strain, the pain was gone after I have put the tape and the athlete was able to play pain-free!!
15. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
Regarding my previous post on 'how to prevent feet of a professional athlete from blisters and serious injuries in the ankle' I wanted to show another great taping technique to support the foot in terms of injury prevention or even if you suffer from an injury like Plantarfasciitis or Metatarsalgia.
Dynamic Tape to support the longitudinal and transverse arch of the foot: in that case the tennis player suffered from a Metatarsalgia. The pain was gone after I have put the tape and the athlete was able to play pain-free!
14. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
INVERSION TRAUMA SERIES 5/5: HOW TO PREVENT FEET FROM INVERSION TRAUMA
The video describes how I prevent the feet of a professional athlete from blisters and serious injuries in the ankle! In the video you can see how I prepare Janko Tipsarevic Official for his singles match at Davis Cup by BNP Paribas competition Serbia vs. Czech Republic.
13. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
INVERSION TRAUMA SERIES 4/5: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE TIBIO TALAR JOINT HVLA
Regarding my previous post about myofascial treatment of the inversion trauma, it is very important to correct the tibiotalar joint if it is still in the wrong position. Usually if you do a proper myofascial release treatment it will correct itself but sometimes it can still stay in the wrong place. If so, there is a high chance to suffer from an ankle dorsiflexion range of motion (DO ROM) deficit which can be reduced significantly through this kind of manipulation!
!!! But watch out: never do this manipulation in the acute phase of an inversion trauma as it can lead to an internal bleeding and edema. To be on the secure side you can apply the HVLA thrust technique 4-5 days after the injury happened!!!
.
The tibiotalar joint involves the talus moving in the ankle mortise, the major motions of this joint are dorsiflexion and plantar flexion. Dorsiflexion is more functional, more stable because the talus is wider anteriorly and fits securely into the ankle mortise. Reduction in dorsiflexion usually indicates that the tibia is anterior on the talus.
The talus usually subluxates anteriorly, superiorly with medial rotation. To reduce the talus subluxation your contact will be on the anterior medial neck of the talus, the elbows will be parallel to each other, the therapist stands in a stable position and applies an high velocity low amplitude thrust technique.
12. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
INVERSION TRAUMA SERIES 3/5: OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE PROXIMAL (SUPERIOR) TIBIOFIBULAR JOINT HVLA PRONE POSITION
Another possibility regarding my previous post about the manipulation of the proximal tibiofibular joint. In this case the patient is laying in prone position and the therapist is using his pisiforme bone of the right hand as a hypomochlion to pull the fibula head to the right position with a high velocity low amplitude (HVLA) thrust technique.
11. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
INVERSION TRAUMA SERIES 2/5: MOBILIZATION AND OSTEOPATHIC MANIPULATION (CHIROPRACTIC ADJUSTMENT) OF THE PROXIMAL (SUPERIOR) TIBIOFIBULAR JOINT HVLA SUPINE POSITION
Regarding my previous post about myofascial treatment of the inversion trauma, it is very important to correct the proximal tibiofibular joint if it is still in the wrong position. Usually if you do a proper myofascial release treatment it will correct itself but sometimes it can still stay in the wrong place. If so, there is a high chance to get lateral knee problems or to force an so-called ascending kinematic chain which even can lead to a wrong position of your pelvis and furthermore to lower back problems, if you don´t work on it properly! Additionally, the patients usually suffer from an ankle DF ROM deficit which can be reduced significantly through this kind of manipulation!
(Treatment technique by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
10. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
INVERSION TRAUMA SERIES 1/5: FASCIAL TREATMENT
If you suffer from inversion trauma of the ankle it is very important to find a therapist who can correct all structures which went into a wrong position (out of balance). When you twist your ankle into inversion, which is the most common injury at the ankle, your anatomical structures, especially the fascias, lead into a wrong position and will stay there if they didn´t get the right treatment to correct them to the right position to achieve the perfect balance!
From the biomechanic few at the inversion trauma your foot closes medially and opens laterally. The lateral part of the lower leg ends up being lengthened (locked long) and the medial part ends up being shortened (locked short). In the video you can see different techniques to correct the fascial structures (including middle tibiofibular ligament/interosseus membrane) and several manual joint techniques which are necessary to bring everything back to physiological balance. The peroneus longus and brevis muscle end up being lengthened you need to shorten them. The tibialis posterior muscle, the flexor digitorum longus muscle and the flexor hallucis longus muscle (Tom, Dig and Harry) end up being shortened you need to lengthen them. The plantar part of the foot closes medially and opens laterally so you need to open it medially and close it laterally. The tibialis anterior muscle must be tested first if locked long or short and shall be mobilized into the right direction accordingly. With that kind of treatment you can achieve a better and even quicker healing, additional it minimizes the risk of getting a chronic problem in the ankle which is very often happening after an injury like that! Through the so-called increasing kinematic chain it even can lead to an posterior tilt of your pelvis and furthermore lead to lower back problems, if you don´t work on it properly!
(Treatment strategy and techniques by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
09. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
MYOFASCIAL RELEASE OF THE JAW JOINT MUSCLES
There are 4 muscles which are basically involved in the movement of the jaw joint: Masseter muscle (Originates at the zygomatic bone and inserts at the mandible), Temporalis muscle (Originates at the temporal bone and inserts at the coronoid process of the mandible), Medial pterygoid muscle (Originates at the lateral pterygoid plate and inserts at the mandible) & Lateral pterygoid muscle (Originates at the sphenoid bone and lateral pterygoid plate and inserts at the mandible). The masseter muscle is the strongest muscle in the human body and can harbour some of the most common triggerpoints. The masseter muscle triggerpoints can lead to referred pain in the head as you can see on the red marked zones in the picture. The masseter muscle can force headache, toothache, tinnitus, bruxism, jaw clenching or TMJ syndrome. The temporalis muscle triggerpoints can lead to headache and toothache as well. The lateral pterygoid muscle triggerpoints can lead to cheek pain (like sinusitis), tinnitus, sore throat and TMJ pain. The medial pterygoid muscle triggerpoints can lead to the same symptoms as the lateral pterygoid. The jaw joint muscles are connected to the suboccipital muscles and shoulder muscles. Triggerpoints in the jaw joint muscles can initiate triggerpoints in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the jaw joint you always have to focus on the cervical spine and shoulder region as well!
On the picture you can see different possibilities of treating the jaw joint muscles intra and extra oral.
P.S.: If you have any dentist treatment, you should always have checked all the muscles which I was talking about after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to problems.

08. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
SEGMENTAL THORACIC AUTOMOBILIZATION EXERCISE WITH THE BLACKROLL®
The thoracic spine is built from its anatomical structure to be mobile! That's why it is very important to keep it mobile and even to visualise and feel the possible movement in the thoracic spine. Many people don't even know or just are not able to feel that there is a specific movement possible, for visualising this movement the Blackroll® is an excellent training device.
Your spine needs to be mobile - our body is smart and will find to get that motion from somewhere else! Those areas of compensation might lead to poor movement patterns, overuse and pain.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain, lower back pain and even hip pain. That´s why it is very important to include this mobilization exercise, together with a pectoralis muscle stretching exercise, in your daily training routine. Because if the pectoralis muscle is locked short it won't be possible to mobilize the thoracic spine properly!
- Roll out your back for 1 minute
- Start with your roller at the beginning of your lumbar spine
- Bend your arms in the elbow and extend over the roller
- Work segmentally up to your cervical spine and then back
- It's ok to pause into the extension and allow your spine to relax over the roller
07. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
MUSCLES WHICH CAN INITIATE HEADACHES - SERIES 5/5: THE SUBOCCIPITAL MUSCLES
There are 4 muscles involved in the suboccipital region also called 'Upper Cervical Spine': Rectus capitis posterior minor, Rectus capitis posterior major, Obliquus capitis inferior and Obliquus capitus superior. These muscles are deeper than all other muscles in the back of the neck and they are very strongly connected to our eyes to give the feedback to the larger neck muscles as to where the head is positioned! The purpose of these muscles is to provide fine motor function in movements of the head. The actions of trapezius, sternocleidomastoid and other larger muscles that move the head are refined by the relatively small suboccipital muscles. As the neck starts to flex in the lower cervical, our eyes always want to look forward, the head and upper cervical spine starts to extend, the suboccipitals shorten and hold the back of the skull to the top two vertebrae (Atlas and Axis) and lock it in place. As I described already in my previous post, these muscles are also a common area to develop trigger points that can cause terrible headaches as you can see on the red marked zones in the picture. Approximately 50% of the neck rotation should come from the first two vertebrae. The rest of the cervical spine splits the other 50%, gradually rotating less and less as you progress from C3 to C7. The suboccipital area is very prone to get stiff and immobile, when the upper cervical spine can't rotate properly, that motion get picked up by the lower cervical spine, which we want to be actually more stable!
(Treatment techniques by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
06. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
MUSCLES WHICH CAN INITIATE HEADACHES - SERIES 4/5: THE TEMPORALIS MUSCLE
The temporalis muscle originates at the temporal bone and inserts at the coronoid process of the mandible, it is a fan shaped muscle on each side of the skull. It is a major muscle involved in moving the temporomandibular joint (Jaw joint muscle). Excess tension here can be a big cause of headaches. This muscle works a lot and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension. The temporalis muscle trigger points can lead to headache and toothache as well. The temporalis muscle is connected to the suboccipital muscles and shoulder muscles. Trigger points in the temporalis can initiate trigger points in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the temporalis you always have to focus on the cervical spine and shoulder region as well:
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to problems.
(Treatment techniques by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
05. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
MUSCLES WHICH CAN INITIATE HEADACHES - SERIES 3/5: THE MASSETER MUSCLE
The masseter muscle (originates at the zygomatic bone and inserts at the mandible) is the strongest muscle in the human body and can harbour some of the most common trigger points. It is a major muscle involved in moving the temporomandibular joint (jaw joint muscle). Excess tension here can be a big cause of headaches. This muscle works a lot and gets brutally tight over time. Clenching the teeth due to things like stress and anxiety will greatly increase this tension. The masseter muscle trigger points can lead to referred pain in the head as you can see on the red marked zones in the picture. The masseter muscle can force headache, toothache, tinnitus, bruxism, jaw clenching or TMJ syndrome. The masseter muscle is connected to the suboccipital muscles and shoulder muscles. Trigger points in the masseter can initiate trigger points in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the masseter you always have to focus on the cervical spine and shoulder region as well!
On the picture you can see several myofascial release techniques for the masseter muscle.
P.S.: If you have any dentist treatment, you should always have checked all the Jaw joint muscles after, as it can lead to exactly those problems mentioned above. Usually they won't appear right on the next day after, as the human body is very good at compensating, but they can appear anytime later on. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer compensate them, it will come to problems!
04. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
Just got in at this beautiful place on the tennis planet: BNP Paribas Open. Definitely the best ATP World Tour Masters tournament of the year! #IndianWells #USA




04. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
MUSCLES WHICH CAN INITIATE HEADACHES - SERIES 2/5: THE STERNOCLEIDOMASTOID MUSCLE
The sternocleidomastoid muscle (SCM) is a paired muscle in the superficial layers of the side of the neck. It is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The muscle tends to be overactive in many people we see. It is commonly recruited to help stabilise the neck/head when we adopt poor postures and positions (forward head posture). It is also an accessory muscle to breathing along with the scalenes, so having poor breathing patterns and habits will cause this muscle to overwork all day long and develop too much tension and trigger points. The SCM trigger points can cause a variety of symptoms including headache and face pain, balance problems, visual disturbances, ear and sinus symptoms, and more body wide symptoms. It is the only muscle that creates such wide spread problems.
The SCM is innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen (a foramen in the base of the skull), where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the SCM. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly.
On the picture you can see several myofascial release techniques for the sternocleidomastoid muscle incl. the Jugular foramen release.
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
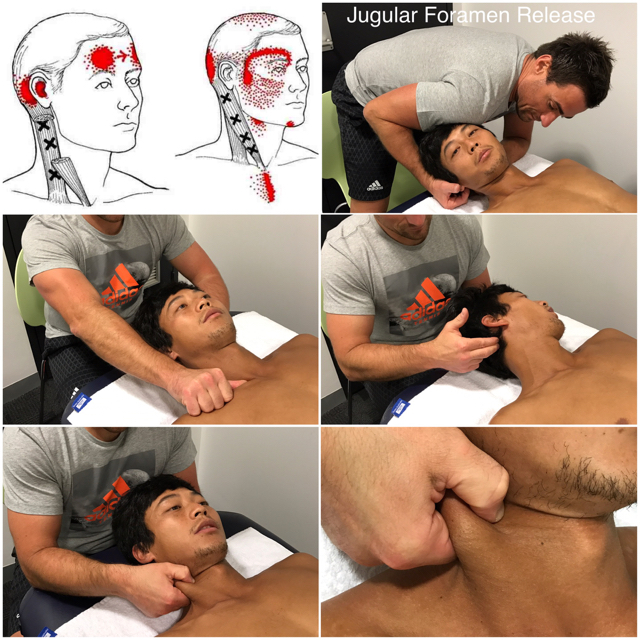
03. March 2017
Indian Wells - BNP Paribas Open - ATP 1000
If you or your patient is suffering from headaches, watch out to my upcomig posts!
MUSCLES WHICH CAN INITIATE HEADACHES - SERIES 1/5: THE TRAPEZIUS MUSCLE
The trapezius muscle is one of the largest superficial muscles that extend longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to the spine of the scapula. Its functions are to move the scapulae and support the arm. The trapezius has three functional regions: the superior region (descending part), which supports the weight of the arm; the intermediate region (transverse part), which retracts the scapulae; and the inferior region (ascending part), which medially rotates and depresses the scapulae. Contraction of the trapezius can have two effects: movement of the scapulae when the spinal origins are stable, and movement of the spine when the scapulae are stable. Its main function is to stabilize and move the scapula.
This muscle tends to develop too much tension for postural reasons, such as forward head posture (where it has to work overtime to stabilise the head and neck due to poor alignment). Other reasons include poor breathing patterns (shallow neck breathing all day), and muscle imbalances elsewhere.
The trapezius muscle trigger points can lead to referred pain in the shoulder region and head (headache) as you can see on the red marked zones in the picture. They also can initiate trigger points in the jaw joint muscles. Additionally, the muscle can cause biomechanical problems in the cervical and thoracic spine.
The trapezius is innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen, where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the trapezius. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly.
(Treatment techniques by Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
01. March 2017
Acapulco - Abierto Mexicano del Tenis - ATP 500
Piriformis Muscle Syndrome (PMS) and Myofascial Treatment
The piriformis is a small, relatively short, and little-known muscle buried deep within the muscle tissue in your hips.
In each hip, it runs from the back of your pelvis to the top of your femur. Because of its unique positioning, the piriformis muscle helps rotate your leg outward when your hip is extended, but rotates your leg inward and into abduction when your hip is flexed.
Your piriformis is positioned immediately adjacent to the sciatic nerve, a very thick nerve which runs from the base of your spine along your glute muscles and down the back of your legs, providing the nerve signals that allow all of the muscles on the back side of your lower body to fire when needed.
When the piriformis muscle is irritated, the sciatic nerve can get irritated too.
In around fifteen percent of people, the sciatic nerve actually passes through the piriformis, which, according to some researchers, leaves these individuals more susceptible to piriformis syndrome.
Symptoms of PMS:
1 - Classically, it feels like an aching, soreness, or tightness in your butt, between the back of your pelvis (the sacrum, specifically) and the top of your femur.
2 - Pain, tightness, tingling, weakness, or numbness can also radiate into your lower back and down the back side of your leg, through your hamstrings and calves.
3 - Buttock pain and tightness with prolonged sitting is also a common occurrence.
4 - When you run, you will probably feel pain in your butt throughout the stance phase of your stride.
Piriformis syndrome is related to sciatica, a painful irritation which also involves pain, tightness, weakness, and a numb or tingling sensation than courses down from your lower back into your butt, hamstring, and calves or even feet.
On the picture you can see several myofascial treatment techniques for the piriformis muscle.
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
28. February 2017
Acapulco - Abierto Mexicano del Tenis - ATP 500
THE POPLITEUS MUSCLE:
The popliteus muscle is a fairly small muscle located behind the knee. It runs from the lateral side of the femur to the medial side of the tibia, lying deep beneath the main calf muscle. Its role is to unlock the knee just after the heel touches the ground when you are walking or running. It also has an important role when running downhill as it assists the posterior cruciate ligament (PCL) in decelerating the femur and preventing its sliding forward on the tibia.
Because of its role in assisting the PCL on downhills, runners can start developing symptoms after an abnormally long hill-training session. People with unstable knees (torn ligaments, torn meniscus, arthritis…) are also prone to develop a popliteus problem because of its important role in stabilizing the knee. The popliteus muscle is kind of a key muscle, if there are any irritations inside or outside the knee happening the popliteus usually reacts with tightness and triggerpoints which can lead to pain situations of the knee.
Popliteus muscle problems remain under-diagnosed to this day, meaning that a lot of runners suffer from it without knowing. Its small role in gait function and its deep location make it unsuspected and underestimated by a lot of health professionals. Also its symptoms are strangely very similar to those of a torn collateral ligament, a torn meniscus or a Patellofemoral Syndrome. So if you have been experiencing knee pain and it does not seem to heal, ask your health professional about the popliteus.
Popliteus muscle problems simply appear as tendonitis, muscle tightness or triggerpoints so it should be treated the same way meaning anti-inflammatory and physio treatment. Especially with fascial and triggerpoint treatments I experienced very good results! Popliteus muscle problems are fairly easy to treat and respond well to treatment, but the challenge remains in the diagnosis… so keep your eyes open!
On the picture you can see several myofascial treatment techniques for the popliteus muscle and its fascia.
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
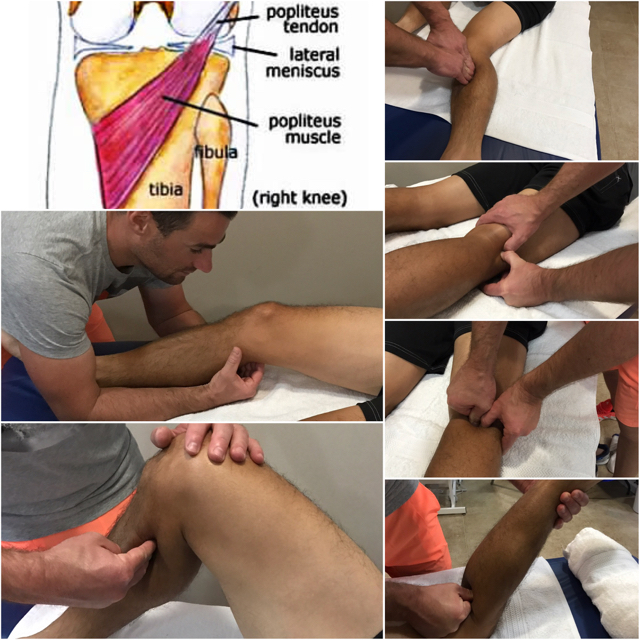
27. February 2017
Acapulco - Abierto Mexicano del Tenis - ATP 500
Just arrived at this beautiful place, unfortunately not for vacation but there are worse places in the world to work at! With Marcelo Meloand Yen-Hsun Rendy Lu the upcoming week in Acapulco at Abierto Mexicano de Tenis.



26. February 2017
Delray Beach - Delray Beach Open - ATP 250
PROTRACTED SHOULDER GIRDLE AND HYPERKYPHOTIC T-SPINE SERIES 5/5:
Another possibility regarding my previous post about the myofascial release of the pectoralis minor muscle:
Out of this position with your thumb you can perform a Triggerpoint technique, a release technique between the fascia of pec major and minor or a release technique for the complete pec minor muscle! If you do the complete pec minor fascial release technique make sure you perform the technique from proximal to distal to lengthen the fascia of the pec major to give the shoulder girdle enough freedom to move back to the right position (Retraction + Depression)!

25. February 2017
Delray Beach - Delray Beach Open - ATP 250
PROTRACTED SHOULDER GIRDLE AND HYPERKYPHOTIC T-SPINE SERIES 4/5:
Another possibility regarding my yesterday's post about the myofascial release of the pectoralis minor muscle. In this case the therapist is moving the arm of the client in abduction and adduction while the elbow of the opposite arm of the therapist is treating the pectoralis minor muscle.
24. February 2017
Delray Beach - Delray Beach Open - ATP 250
PROTRACTED SHOULDER GIRDLE AND HYPERKYPHOTIC T-SPINE SERIES 3/5:
Regarding my previous post about the Protracted Shoulder Girdle, Hyperkyphotic T-Spine and Automobilization with the @BLACKROLL® and BLACKROLL® BALL I wanted to show some treatment techniques to my colleagues on how to work on that problem:
Role of the pectoralis minor muscle?
The pectoralis minor runs from the coracoid process down to ribs 3-5. It will become adaptively short when sitting at the desk, working with computers, favor exercises such as the bench press or other pressing exercises etc., which most people do! Being in poor positions and using the pecs will cause this adaptative shortening and tightness. When the pec minor is positioned short or tight it will pull down on the scapula tilting it forward. It also will inhibit (weaken) the rhomboids, lower trapezius and serratus anterior which will lead to muscular imbalances!
In the video you can see a myofascial release technique for the pectoralis minor muscle.
23. February 2017
Delray Beach - Delray Beach Open - ATP 250
PROTRACTED SHOULDER GIRDLE AND HYPERKYPHOTIC T-SPINE SERIES 2/5:
Regarding my yesterdays post about the Protracted Shoulder Girdle, Hyperkyphotic T-Spine and Automobilization with the Blackroll® and BLACKROLL® BALL I wanted to show some treatment techniques to my colleagues on how to work on that problem:
In the video you can see a myofascial release technique for the pectoralis major muscle. It is very important to perform the fascial technique from proximal to distal to lengthen the fascia of the pec major to give the shoulder girdle enough freedom to move back to the right position (Retraction + Depression)!
(Treatment technique: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
22. February 2017
Delray Beach - Delray Beach Open - ATP 250
PROTRACTED SHOULDER GIRDLE AND HYPERKYPHOTIC T-SPINE SERIES 1/5:
Protracted Shoulder Girdle, Hyperkyphotic T-Spine and Automobilization with the BLACKROLL® and Blackroll® BALL:
Why your shoulders and thoracic spine are rounded?
Many people suffer nowadays from this alignment which is caused mainly by 2 key-muscles: 1 - the pectoralis minor and 2 - the lower trapezius muscle (ascending part of the trapezius).
1 - The pectoralis minor runs from the coracoid process down to ribs 3-5. It will become adaptively short when sitting at the desk, working with computers etc., which most people do! Being in poor positions and using the pecs will cause this adaptative shortening and tightness. When the pec minor is positioned short it will pull down on the scapula tilting it forward.
2 - The lower trapezius runs from vertebra T7-T12 up to the spine of the scapula. Normally this muscle pulls down on the scapula from the back creating a balancing act with the pectoralis minor for the scapula position. But if the pec minor is getting tight and short throughout poor positioning the lower trap gives up and gets weaker and weaker!
This poor alignment we are talking about can even lead to mechanical problems in the cervical spine or shoulder joint as it makes it very difficult to use the glenohumeral joint in centrated neutral position. That's why it is essential to work on it!
On the picture you can see different possibilities how to work by yourself on this problems with the BLACKROLL® and BLACKROLL® BALL releasing the pec minor and 2 variations of mobilizing your thoracic spine as well as 1 exercise to put some in the lower trap to activate it!

21. February 2017
Delray Beach - Delray Beach Open - ATP 250
Great comeback today Rendy from 4:6 and 0:3 down.

20. February 2017
Delray Beach - Delray Beach Open - ATP 250
THORACIC OUTLET SYNDROME SERIES 4/4:
Regarding my previous post about the Thoracic Outlet Syndrome (TOS) I wanted to show some treatment techniques to my colleagues on how to solve the COSTOCLAVICULAR SYNDROME - MYOFASCIAL RELEASE OF THE SCALENE MUSCLES AND SUBCLAVIUS MUSCLE AS WELL AS MOBILIZATION OF THE FIRST RIB AND THORACIC SPINE:
Symptoms result in this case when the neurovascular bundle is tractioned between the clavicle and the first rib. This is often bilateral, indicating a symmetrical postural cause.
On the picture you can see several myofascial release techniques for the scalene muscles and the subclavius muscle as well as a manual mobilization of the first rib and thoracic spine.
#Physiotherapy #Osteopathy

19. February 2017
Delray Beach - Delray Beach Open - ATP 250
THORACIC OUTLET SYNDROME SERIES 3/4:
Regarding my previous post about the Thoracic Outlet Syndrome (TOS) I wanted to show some techniques to my colleagues on how to solve the PECTORALIS MINOR SYNDROME - MYOFASCIAL RELEASE OF THE PECTORALIS MINOR MUSCLE:
In this case, the compression occurs where the neurovascular bundle passes between the tendon of pectoralis minor and the coracoid process of the scapula. Tractioning is greatest with the arm in abduction, but even with the arm dependent, enough pressure frompostural problems or tight pectoralis muscles can cause symptoms.
On the picture you can see several myofascial release techniques for the pectoralis minor muscle.

18. February 2017
Delray Beach - Delray Beach Open - ATP 250
THORACIC OUTLET SYNDROME SERIES 2/4:
Regarding my yesterday's post about the Thoracic Outlet Syndrome (TOS) I wanted to show some techniques to my colleagues on how to solve the SCALENE ANTERIOR SYNDROME - MYOFASCIAL RELEASE OF THE SCALENE MUSCLES AND STERNOCLEIDOMASTOID MUSCLE:
Anatomy:
The fibres of the brachial plexus and the subclavian artery must pass through a narrow aperture between anterior and middle scalene muscle. If this aperture makes a problem it can lead to paresthesia or weaknessin the upper limb.
The fibres of the subclavian vein, the suprascapular vein, the transverse cervical vein and the phrenic nerve must pass through a narrow aperture between the anterior scalene muscle and the sternocleidomastoid muscle. If this aperture makes a problem it can lead to edema in the hands/fingers and also to problems with the thoracic diaphragm.
The fibres of the long thoracic nerve must pass through a narrow aperture between middle and posterior scalene muscle. If this aperture makes a problem it can lead to a problem with the serratus anterior muscle.
Any increased tone in one of these muscles (usually scalene anterior), will provide enough compression to produce symptoms. Scarring and adhesions from injuries can be causes of compression, particularly if found at the attachments of the scalenes. Dysfunction or misalignent of the cervical spine may also be a contributing factor to this syndrome.
On the picture you can see several myofascial release techniques for the scalene muscles as well as for the sternocleidomastoid muscle.
#Physiotherapy #Osteopathy
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)

17. February 2017
Delray Beach - Delray Beach Open - ATP 250
THORACIC OUTLET SYNDROME SERIES 1/4:
The Thoracic Outlet Syndrome (TOS) and Automobiization (Self-Treatment):
TOS are a group of syndromes involving pressure on the brachial plexus.
Each syndrome is named according the structure that is causing the compression.
SCALENE ANTERIOR SYNDROME:
The fibres of the brachial plexus must pass through a narrow aperture between scalenes anterior and medius. Any increased tone in one of these muscles (usually anterior), will provide enough compression to produce symptoms. Scarring and adhesions from injuries can be causes of compression, particularly if found at the attachments of the scalenes. Dysfunction or misalignent of the cervical spine may also be a contributing factor to this syndrome.
PECTORALIS MINOR SYNDROME (HYPERABDUCTION SYNDROME): In this case, the compression occurs where the neurovascular bundle passes between the tendon of pectoralis minor and the coracoid process of the scapula. Tractioning is greatest with the arm in abduction, but even with the arm dependent, enough pressure from postural problems or tight pectoralis muscles can cause symptoms.
COSTOCLAVICULAR SYNDROME:
Symptoms result in this case when the neurovascular bundle is tractioned between the clavicle and the first rib. This is often bilateral, indicating a symmetrical postural cause.
CAUSES:
Crutch use; Joint subluxation; Adhesions and scarring; Muscular hypertonicity from postural dysfunction such as hyperkyphosis, trigger points, occupational stresses, emotion stresses, all of which lead to shallow breathing, and poor sleeping posture.
SIGNS AND SYMPTOMS:
All thoracic outlet syndromes feature paraesthesia in the arm, forearm, hand, and fingers. Symptoms are usually unilateral, but can be bilateral, particularly if postural dysfunction is a main cause.
Anterior scalene syndrome is also noted for edema in the hands and fingers.
On the picture you can see several exercises which can help if you suffer from TOS:
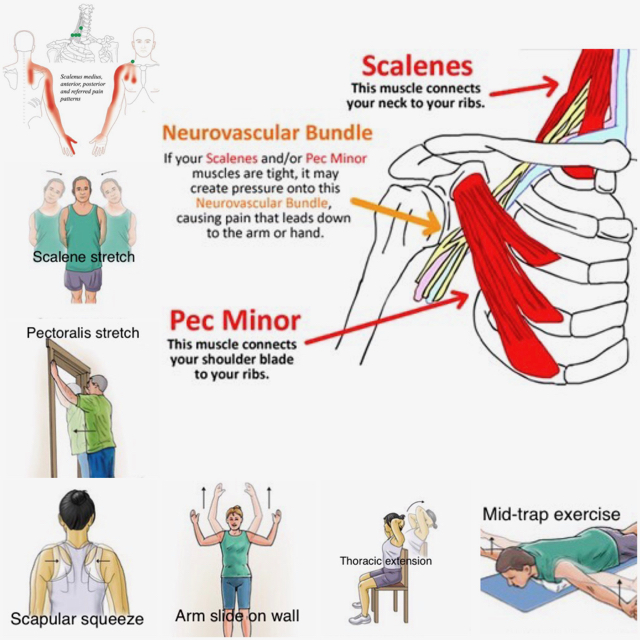
13. February 2017
Memphis - Memphis Open - ATP 250
Centre Court:

Cryo-Therapy:

12. February 2017
Memphis - Memphis Open - ATP 250
Piriformis Muscle Syndrome (PMS) and Automobilization (Self-Treatment):
The piriformis is a small, relatively short, and little-known muscle buried deep within the muscle tissue in your hips.
In each hip, it runs from the back of your pelvis to the top of your femur. Because of its unique positioning, the piriformis muscle helps rotate your leg outward when your hip is extended, but rotates your leg inward and into abduction when your hip is flexed.
Your piriformis is positioned immediately adjacent to the sciatic nerve, a very thick nerve which runs from the base of your spine along your glute muscles and down the back of your legs, providing the nerve signals that allow all of the muscles on the back side of your lower body to fire when needed.
When the piriformis muscle is irritated, the sciatic nerve can get irritated too.
In around fifteen percent of people, the sciatic nerve actually passes through the piriformis, which, according to some researchers, leaves these individuals more susceptible to piriformis syndrome.
Symptoms of PMS:
Classically, it feels like an aching, soreness, or tightness in your butt, between the back of your pelvis (the sacrum, specifically) and the top of your femur.
Pain, tightness, tingling, weakness, or numbness can also radiate into your lower back and down the back side of your leg, through your hamstrings and calves.
Buttock pain and tightness with prolonged sitting is also a common occurrence.
When you run, you will probably feel pain in your butt throughout the stance phase of your stride.
Piriformis syndrome is related to sciatica, a painful irritation which also involves pain, tightness, weakness, and a numb or tingling sensation than courses down from your lower back into your butt, hamstring, and calves or even feet.
On the picture you can see different possibilities how to work by yourself on releasing the piriformis muscle.
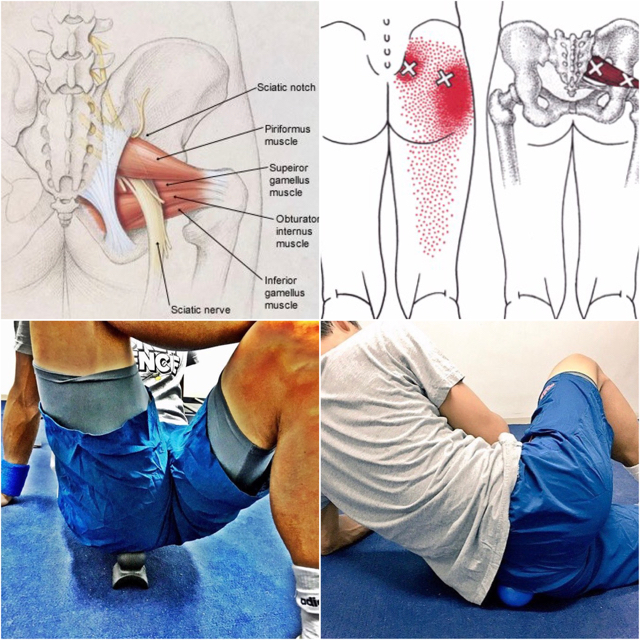
10. February 2017
Memphis - Memphis Open - ATP 250
How good is that!? Checked in at my hotel and at the reception is a delivery from Bounce Canada waiting. Thank you guys, really appreciate it!


09. February 2017
Memphis - Memphis Open - ATP 250
On the ✈️ to USA for the next ATP World Tour work journey. Upcoming destinations are Memphis (Memphis Open), Delray Beach (Delray Beach Open), Acapulco (Abierto Mexicano de Tenis), Indian Wells (BNP Paribas Open) and Miami (Miami Open).
07. February 2017
HAMMER SPORT AG Article
Thank you HAMMER SPORT AG for interviewing me and featuring an article about "muscular dysbalances in tennis" in their current issue!
Vielen Dank an Hammer Sport AG für das Interview und die Veröffentlichung eines Artikels über "Muskuläre Dysbalancen im Tennis"!
http://www.hammer.de/…/richtig-…/bilaterales-training-tennis
05. February 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Davis Cup Match Day 3: Dusan vs. Kravchuk
Match preparation for Dutzi :-)

04. February 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Davis Cup Match Day 2 Doubles: Viktor/Nenad vs. Kravchuk/Kuznetsov








03. February 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Davis Cup Match Day 1 Singles: Viktor vs. Khachanov and Novak vs. Medvedev












02. February 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Davis Cup Team Serbia at official draw ceremony today #Davis Cup by BNP Paribas #TeamSerbia




01. February 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Official Davis Cup Dinner at World Group 1st Round tie Serbia vs. Russia #Davis Cup by BNP Paribas #TeamSerbia
(Picture Credit: Teniski savez Srbije)

31. January 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Incredible team spirit in the Serbian Davis Cup by BNP Paribas Team, proud to be one part of it!
#SRBRUS #TeamSRB #Physiotherapist #TeamSpirit

30. January 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
In Niš/Serbia for World Group 1st Round Davis Cup by BNP Paribas tie Serbia vs. Russia #TeamSerbia

29. January 2017
Nis/Serbia - Davis Cup - 1st Round Serbia vs. Russia
Looking forward to join the serbian Davis Cup team in a few hours... on my way to Belgrade to support the team at the 1st Round tie Serbia vs. Russia. Proud to be a member of one of the best national tennis teams of the world, let´s go! #DavisCup #SERvsRUS #OfficialPhysiotherapist #TeamSpirit

28. January 2017
Donaustauf/Regensburg - Eden Reha - Faszientherapeutische Arbeit im Spitzensport
The Master himself at work: Robert Schleip demonstrating a myofascial release technique of the lumbar fascia (2nd layer) - very effective if you suffer from lower back problems!
#Rolfing #MyofascialRelease #Bodywork #Physiotherapy #Osteopathy
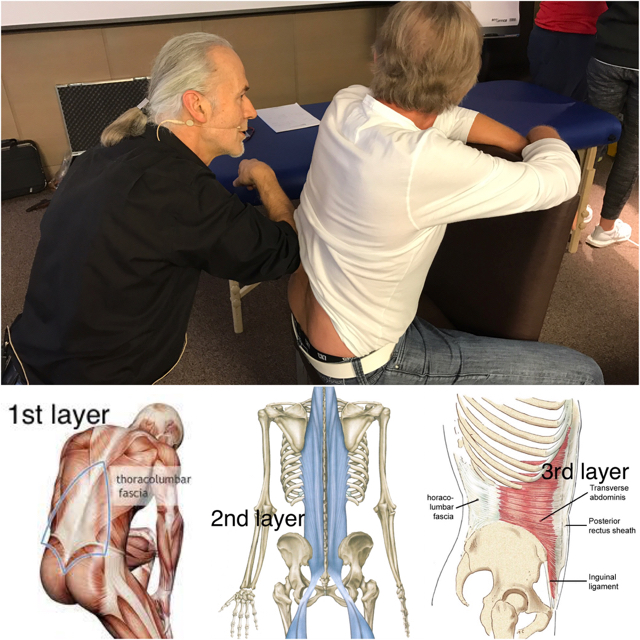
27. January 2017
Donaustauf/Regensburg - Eden Reha - Faszientherapeutische Arbeit im Spitzensport
Just arrived back form Melbourne/Australian Open and got very lucky to catch a spot in a 2 day course regarding the newest techniques of fascial treatment in professional sports provided by two legends in their job: Klaus Eder, Physiotherapist for DFB-Team (Die Mannschaft) and Davis Cup by BNP Paribas Team Germany: One of the most important persons responsible for my own physio career with all his knowledge he provided to me and basically opened the door for me to start working in professional tennis 10 years ago! Dr. biol. hum. Robert Schleip (PhD), International Rolfing® Instructor and International Fascial Anatomy Teacher, one of the most important persons regarding #FasciaResearchworldwide: www.fasciaresearch.de! Always a pleasure to listen to this guys. Thank you to EDEN REHA for letting me attend in last minute!
#Physiotherapy #Osteopathy #FascialTreatment

24. January 2017
Melbourne - Australian Open - Grand Slam
Always a pleasure to do physiotherapy treatment with Boris Becker! #ChildhoodHero #WhenDreamsComeTrue

19. January 2017
Melbourne - Australian Open - Grand Slam
MYOFASCIAL RELEASE OF THE TRAPEZIUS AND STERNOCLEIDOMASTOID MUSCLE (SCM):
The trapezius muscle is one of the largest superficial muscles that extend longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to the spine of the scapula. Its functions are to move the scapulae and support the arm. The trapezius has three functional regions: the superior region (descending part), which supports the weight of the arm; the intermediate region (transverse part), which retracts the scapulae; and the inferior region (ascending part), which medially rotates and depresses the scapulae. Contraction of the trapezius muscle can have two effects: movement of the scapulae when the spinal origins are stable, and movement of the spine when the scapulae are stable. Its main function is to stabilize and move the scapula.
The trapezius muscle triggerpoints can lead to referred pain in the shoulder region and head as you can see on the red marked zones in the picture. Additionally, the muscle can cause biomechanical problems in the cervical and thoracic spine. Trapezius muscle and SCM triggerpoints can initiate triggerpoints in the jaw joint muscles.
The sternocleidomastoid muscle (SCM) is a paired muscle in the superficial layers of the side of the neck. It is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The SCM triggerpoints can cause a variety of symptoms including head and face pain, balance problems, visual disturbances, ear and sinus symptoms, and more body wide symptoms. It is the only muscle that creates such wide spread problems.
Both muscles are innervated by the accessory nerve (Cranial nerve XI) which is content of the jugular foramen (a foramen in the base of the skull), where the accessory nerve can get compressed or entrapped. If so, it can lead to hypertension in the trapezius and SCM. That's why it is very important to treat (release) this foramen to give the nerve enough space to work properly. On the picture, you can see the jugular foramen release technique as well as several myofascial release techniques for both muscles.
#Physiotherapy #Osteopathy
(Treatment techniques: Lutz M. Scheuerer - Deutsches Fortbildungsinstitut für Osteopathie)
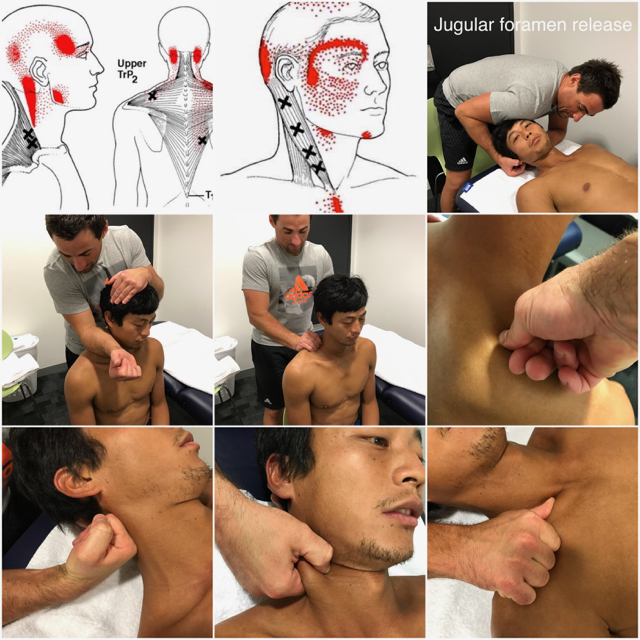
17. January 2017
Melbourne - Australian Open - Grand Slam
MYOFASCIAL RELEASE OF THE SUBOCCIPITAL MUSCLES AND OSTEOPATHIC MANIPULATION OF THE OAA COMPLEX HVLA:
There are 4 muscles involved in the suboccipital region also called 'Upper Cervical Spine': Rectus capitis posterior minor, Rectus capitis posterior major, Obliquus capitis inferior and Obliquus capitus superior. These muscles are deeper than all other muscles in the back of the neck and they are very strongly connected to our eyes to give the feedback to the larger neck muscles as to where the head is positioned!
The purpose of these muscles is to provide fine motor function in movements of the head. The actions of trapezius, sternocleidomastoid and other larger muscles that move the head are refined by the relatively small suboccipital muscles.
As the neck starts to flex in the lower cervical, our eyes always want to look forward, the head and upper cervical spine starts to extend, the suboccipitals shorten and hold the back of the skull to the top two vertebrae (Atlas and Axis) and lock it in place. As I described already in my previous post, these muscles are also a common area to develop trigger points that can cause terrible headaches. Another cause for headaches can be a suboccipital nerve entrapment (Occipital neuralgia). The nerve is content of the suboccipital triangle bounded by the Rectus capitis posterior major, the Obliquus capitis superior and the Obliquus capitis inferior. The nerve may become entrapped beneath the attachments of the trapezius and semispinalis capitis muscles to the occipital bone especially if the Occiput-Altlas-Axis-Complex (OAA) is in the wrong position. Approximately 50% of the neck rotation should come from the first two vertebrae. The rest of the cervical spine splits the other 50%, gradually rotating less and less as you progress from C3 to C7. The suboccipital area is very prone to get stiff and immobile, when the upper cervical spine can't rotate properly, that motion get picked up by the lower cervical spine, which we want to be actually more stable! On the picture you can see several myofascial release techniques for the suboccipital muscles as well as a mobilization technique for the upper cervical spine to flexion and a Osteopathic Manipulation of the Occiput-Atlas-Axis-Complex (OAA) using the Chin-Hold-Technique (HVLA). Usually if you do a proper myofascial release treatment, the Occiput-Atlas-Axis-Complex (OAA) will get into the right position by itself. If not, it requires a high velocity low amplitude (HVLA) thrust technique! In this case the Atlas had a shift lesion to the right.
#Physiotherapy #Osteopathy




15. January 2017
Melbourne - Australian Open - Grand Slam
MYOFASCIAL RELEASE OF THE JAW JOINT MUSCLES:
There are 4 muscles which are basically involved in the movement of the jaw joint: Masseter muscle (Originates at the zygomatic bone and inserts at the mandible), Temporalis muscle (Originates at the temporal bone and inserts at the coronoid process of the mandible), Medial pterygoid muscle (Originates at the lateral pterygoid plate and inserts at the mandible) & Lateral pterygoid muscle (Originates at the sphenoid bone and lateral pterygoid plate and inserts at the mandible). The masseter muscle is the strongest muscle in the human body and can harbour some of the most common triggerpoints. The masseter muscle triggerpoints can lead to referred pain in the head as you can see on the red marked zones in the picture. The masseter muscle can force headache, toothache, tinnitus, bruxism, jaw clenching or TMJ syndrome. The temporalis muscle triggerpoints can lead to headache and toothache as well (red zones in the picture). The lateral pterygoid muscle triggerpoints can lead to cheek pain (like sinusitis), tinnitus, sore throat and TMJ pain. The medial pterygoid muscle triggerpoints can lead to the same symptoms as the lateral pterygoid. The jaw joint muscles are connected ⛓to the suboccipital muscles and shoulder muscles. Triggerpoints in the jaw joint muscles can initiate triggerpoints in the suboccipital muscles and shoulder region (esp. in the trapezius muscle). That means whenever you treat the jaw joint you always have to focus on the cervical spine and shoulder region as well! I will show in my next post how to treat the suboccipital region and the trapezius muscle.
On the picture you can see different possibilities of treating the jaw joint muscles intra and extra oral.
P.S.: If you have any dentist treatment, you should always have checked all the muscles which I was talking about after, as in the long-run, it can lead to exactly those problems mentioned above, or even cervical spine or shoulder problems. Usually they won't (but could) appear right on the next day after dental treatment, as the human body is very good at compensating, but they can appear anytime later on, especially if you have further dental treatments. Each single dental treatment is a kind of a micro-trauma, and if the body can no longer process or compensate them, it will come to a big problem!

14. January 2017
Melbourne - Australian Open - Grand Slam
You suffer from lower back pain?
Add foam rolling to your workout! It is very helpful and supports myofascial treatment to reduce the fascial tension in TFL muscle and IT band which can cause an outflare ilium and additionally a sacrum contranutation, that leads to an asymmetric position (hypolordosis) in the lumbar spine and to lower back problems! #Blackroll®

13. January 2017
Melbourne - Australian Open - Grand Slam
Just checked in at Australian Open, the best Grand Slam of the year!
10. January 2017
Auckland - ASB Classic - ATP 250
MYOFASCIAL RELEASE OF THE SUBCLAVIUS MUSCLE
The subclavius muscle is a short muscle of the shoulder girdle. It originates at the first rib (border between the bone and cartilage) and inserts at the lower surface of the lateral clavicle. The main task of the subclavius muscle is the active stabilization of the clavicle in the sternoclavicular joint during movements of the shoulder and arm. Furthermore its contraction leads to a depression of the clavicle and elevation of the first rib respectively.
Its importance lies in the fact that it can influence the movement and position of the shoulder joint.
Despite its importance, the subclavius isn’t well known or appreciated which is very unfortunate, as in my experience it is a very important muscle to have always in focus, especially if your patient is suffering from shoulder or cervical spine problems!
Once you understand its position and actions, it is not surprising that the subclavius can be a source of shoulder pain, not only because it is sore or hurt, but because when it gets too tight it can pull the shoulder forward and down, thus misaligning the shoulder joint. Any time the gleno-humeral joint, sterno-clavicular joint or acromio-clavicular joint aren't aligned properly, pain can arise. The subclavius muscle triggerpoint can lead to referred pain in the arm as you can see on the red marked zones in the picture. Additionally, the muscle can cause biomechanical problems in the cervical spine, due to its influence on the first rib in terms of elevating it, as the rotation in the cervical spine will be irritated.
On the picture you can see different possibilities of treating the subclavius muscle.
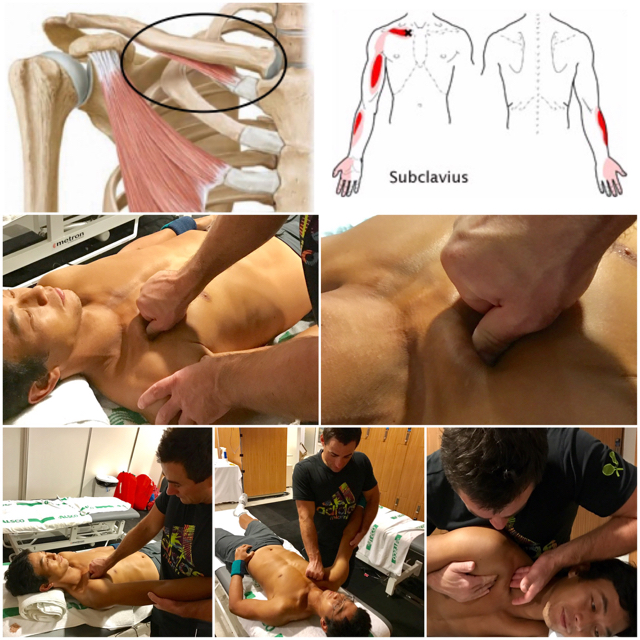
09. January 2017
Auckland - ASB Classic - ATP 250
FOAM ROLLING with the BLACKROLL on important structures which can force lower back, hip, knee and foot problems:
Some general information about foam rolling on the important muscles which keep the ilium bone in the anterior rotated position regarding my post on 5th of January: 'Osteopathic Manipulation of the Sacroiliac Joint using the Chicago Technique HVLA'.
How to perform a self myofascial release (self massage) to your muscles? Every foam rolling fanatic knows how to do it but it is very important to make sure to spend time on each of the individual muscles which keep the ilium bone in anterior rotated position (Iliacus muscle, Erector spinae muscles, Latissimus dorsi muscle, Adductor muscles, Rectus femoris muscle, Quadratus lumborum muscle, Tensor fascia latae muscle, gluteus medius muscle and External obturator muscle).
Make sure that you roll slowly among each muscle, trying to identify areas of tightness or discomfort. Pause on these areas for several seconds and the tightness should begin to ease. Continue this process on each muscle until it feels as though you have an improvement or a decrease in general tightness. Ensuring you roll each muscle from the origin to the insertion is a good way to target the entire length of the muscle.

08. January 2017
Auckland - ASB Classic - ATP 250
Center Court:

Segmental Thoracic Automobilization Exercise with the Blackroll
The thoracic spine is built from its anatomical structure to be mobile! That's why it is very important to keep it mobile and even to visualise and feel the possible movement in the thoracic spine. Many people don't even know or just are not able to feel that there is a specific movement possible, for visualising this movement the BLACKROLL is an excellent training device.
An immobility or stiffness in the thoracic spine can lead to rounded shoulders, shoulder pain, elbow pain, wrist pain, neck pain and even lower back pain. That´s why it is very important to include this mobilization exercise, together with a pectoralis muscle stretching exercise in your daily training routine. Because if the pectoralis muscle is locked short it won't be possible to mobilize the thoracic spine properly!
07. January 2017
Auckland - ASB Classic - ATP 250
Walking around and trying to kill Mr. JetlagWalking around and trying to kill Mr. Jetlag after a 24h trip #Chennai #Dubai #Auckland #NewZealand #ASB Classic #ATP World Tour

06. January 2017
Chennai - Aircel Chennai Open - ATP 250
Thank you Aircel Chennai Open, it was a great week supporting Yen-Hsun Rendy Lu and Andre Begemann in an amazing city. Ready for a 24h trip to Auckland for ASB Classic, next tournament of 2017 ATP World Tour season!

